[level-membership-for-anesthesiology-category]
38 Lateral Femoral Cutaneous Nerve Block
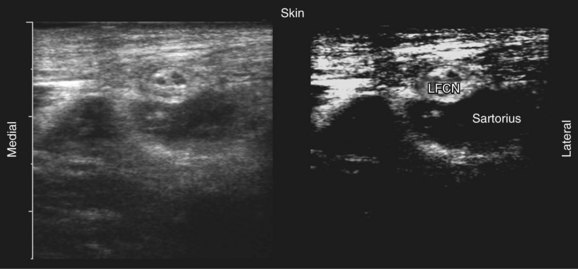
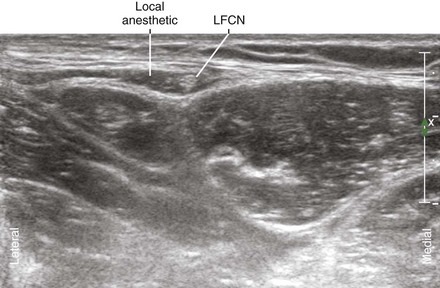
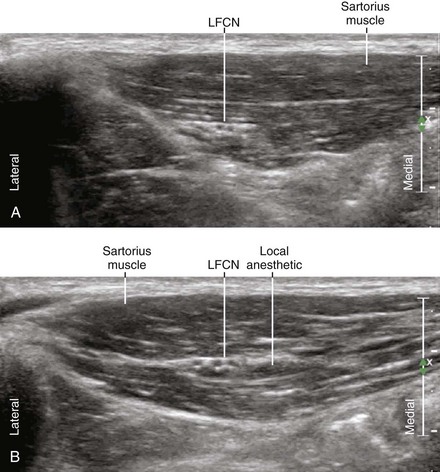
High-resolution ultrasound imaging can identify the LFCN superficial to the sartorius muscle in the proximal thigh.1,2 The nerve has a characteristic medial to lateral course over this muscle. The nerve and muscle are best visualized just medial and distal to the ASIS. As with other small nerves, it is necessary to scan along the length of the nerve to confirm nerve identity. The best imaging technique is to slide the transducer along the known course of the nerve with the nerve viewed in short axis. LFCNs that pass through the sartorius are easier to image because the nerve is surrounded by hypoechoic muscle that provides better acoustic contrast than echobright subcutaneous tissue. Although ultrasound imaging of the LFCN has been reported, the nerve is normally small (1-3 mm in diameter), and sonographic visualization can be difficult within the echobright subcutaneous tissue of the anterior thigh.
LFCN block can be used alone or in conjunction with other lower extremity blocks. It is useful for skin graft harvests and surgical procedures with lateral incisions of the thigh. It is one of the few lower extremity blocks for weight-bearing patients (this group also includes ankle block and saphenous block). LFCN block can improve thigh tourniquet tolerance when combined with other lower extremity blocks.3
Ultrasound imaging may be useful for the diagnosis and treatment of meralgia paresthetica (from Greek meros for “thigh,” and algos for “pain”). Meralgia can result from mechanical stretch or compression injury of the LFCN. Abnormal nerve morphology has been described in patients with meralgia paresthetica. Fusiform enlargement of the LFCN, loss of fascicular discrimination, and hyperemia can all occur in this condition.4–6
Suggested Technique
Key Points
| Lateral Femoral Cutaneous Nerve Block | The Essentials |
|---|---|
| Anatomy | The LFCN usually crosses over the Sa. |
| The LFCN lies in the space between the Sa and TFL. | |
| The Sa is usually triangularly shaped near its ASIS insertion. | |
| The LFCN is about 2.5 mm in diameter. | |
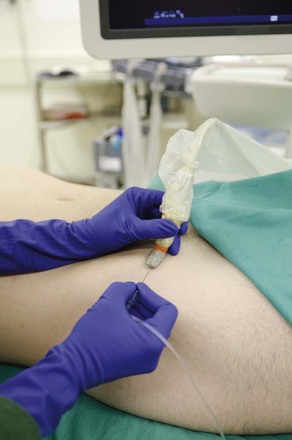
| Positioning | Supine |
| Operator | Standing on side of patient |
| Display | Across the table |
| Transducer | High-frequency linear, 23- to 38-mm footprint |
| Initial depth setting | 20 mm |
| Needle | 25 gauge, 38 mm in length |
| Anatomic location | Proximal lateral thigh, 1 to 2 cm distal to ASIS |
| Begin by sliding transducer back and forth (proximal and distal). | |
| Look for LFCN crossing over the Sa | |
| Approach | SAX view of LFCN, in-plane from lateral to medial |
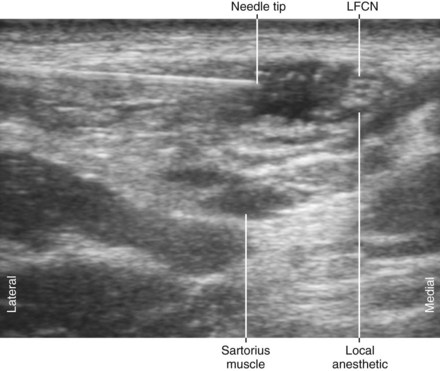
| Place the needle tip between the LFCN and Sa. | |
| Alternatively, place needle tip in space between Sa and TFL. | |
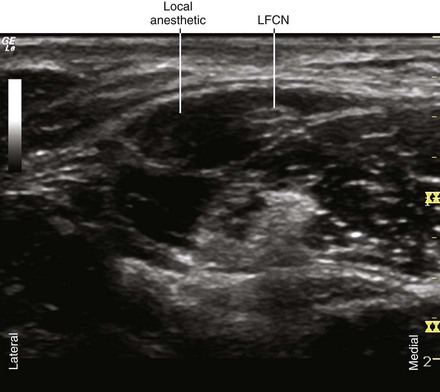
| Sonographic assessment | The injection should track distally along the LFCN. |
| Anatomic variation | The LFCN can travel through the Sa. |
| The LFCN can divide proximally and be difficult to visualize. |
Clinical Pearls
• The LFCN can be imaged between the fascia iliaca and the fascia lata. If light probe pressure is applied, the nerve can be seen within the tissue between these two fascial layers for needle tip placement.7
• LFCN block is assessed by cutaneous anesthesia midway between the ASIS and the lateral knee joint line.
• In some patients the crossing of the LFCN with the deep circumflex iliac artery can be identified on sagittal oblique sonograms.8 This view is parallel to the course of the nerve and perpendicular to the course of the artery.
1 Thain LM, Downey DB. Sonography of peripheral nerves: technique, anatomy, and pathology. Ultrasound Q. 2002;18:225–245.
2 Van Holsbeeck M, Introcaso JH. Musculoskeletal ultrasound, 2nd ed, St. Louis: Mosby, 2001.
3 Morin AM, Pandurovic M, Eberhart LH, et al. Is a blockade of the lateral cutaneous nerve of the thigh an alternative to the classical femoral nerve blockade for knee joint arthroscopy? A randomised controlled study. Anaesthesist. 2005;54:991–999.
4 Hurdle MF, Weingarten TN, Crisostomo RA, et al. Ultrasound-guided blockade of the lateral femoral cutaneous nerve: technical description and review of 10 cases. Arch Phys Med Rehabil. 2007;88:1362–1364.
5 Tumber PS, Bhatia A, Chan VW. Ultrasound-guided lateral femoral cutaneous nerve block for meralgia paresthetica. Anesth Analg. 2008;106:1021–1022.
6 Tagliafico A, Serafini G, Lacelli F, et al. Ultrasound-guided treatment of meralgia paresthetica (lateral femoral cutaneous neuropathy): technical description and results of treatment in 20 consecutive patients. J Ultrasound Med. 2011;30(10):1341–1346.
7 Ng I, Vaghadia H, Choi PT, et al. Ultrasound imaging accurately identifies the lateral femoral cutaneous nerve. Anesth Analg. 2008;107:1070–1074.
8 Damarey B, Demondion X, Boutry N, et al. Sonographic assessment of the lateral femoral cutaneous nerve. J Clin Ultrasound. 2009;37:89–95.
[/level-membership-for-anesthesiology-category][not-level-membership-for-anesthesiology-category]
38 Lateral Femoral Cutaneous Nerve Block
High-resolution ultrasound imaging can identify the LFCN superficial to the sartorius muscle in the proximal thigh.1,2 The nerve has a characteristic medial to lateral course over this muscle. The nerve and muscle are best visualized just medial and distal to the ASIS. As with other small nerves, it is necessary to scan along the length of the nerve to confirm nerve identity. The best imaging technique is to slide the transducer along the known course of the nerve with the nerve viewed in short axis. LFCNs that pass through the sartorius are easier to image because the nerve is surrounded by hypoechoic muscle that provides better acoustic contrast than echobright subcutaneous tissue. Although ultrasound imaging of the LFCN has been reported, the nerve is normally small (1-3 mm in diameter), and sonographic visualization can be difficult within the echobright subcutaneous tissue of the anterior thigh.
LFCN block can be used alone or in conjunction with other lower extremity blocks. It is useful for skin graft harvests and surgical procedures with lateral incisions of the thigh. It is one of the few lower extremity blocks for weight-bearing patients (this group also includes ankle block and saphenous block). LFCN block can improve thigh tourniquet tolerance when combined with other lower extremity blocks.3
Ultrasound imaging may be useful for the diagnosis and treatment of meralgia paresthetica (from Greek meros for “thigh,” and algos for “pain”). Meralgia can result from mechanical stretch or compression injury of the LFCN. Abnormal nerve morphology has been described in patients with meralgia paresthetica. Fusiform enlargement of the LFCN, loss of fascicular discrimination, and hyperemia can all occur in this condition.4–6
