CHAPTER 34 Larynx
The larynx is an air passage, a sphincter and an organ of phonation, and extends from the tongue to the trachea. It projects ventrally between the great vessels of the neck and is covered anteriorly by skin, fasciae and the hyoid depressor muscles. Above, it opens into the laryngopharynx and forms its anterior wall; below, it continues into the trachea (see Fig. 33.2). It is mobile on deglutition. At rest, the larynx lies opposite the third to sixth cervical vertebrae in adult males; it is somewhat higher in children and adult females. In infants between 6 and 12 months, the tip of the epiglottis (the highest part of the larynx) lies a little above the junction of the dens and body of the axis vertebra. Until puberty, male and female larynges are similar in size. After puberty, the male larynx enlarges considerably in comparison with that of the female: all the cartilages increase in both size and weight, the thyroid cartilage projects in the anterior midline of the neck, and its sagittal diameter nearly doubles. The male thyroid cartilage continues to increase in size until 40 years of age, after which no further growth occurs.
SKELETON OF THE LARYNX
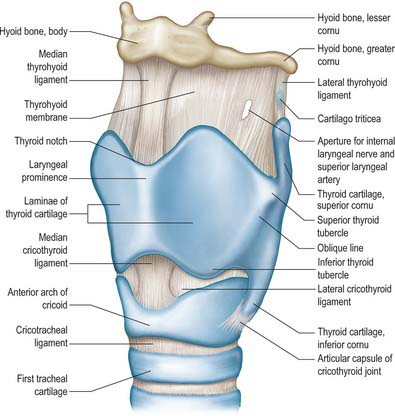
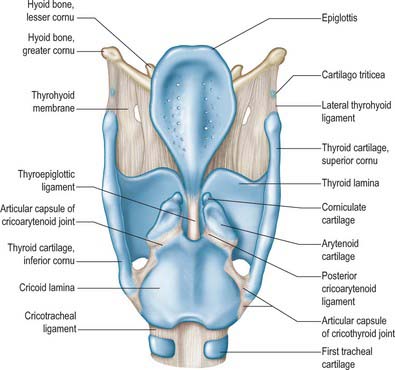
The skeletal framework of the larynx is formed by a series of cartilages interconnected by ligaments and fibrous membranes, and moved by a number of muscles (Figs 34.1–34.3). The hyoid bone is attached to the larynx: it is usually regarded as a separate structure with distinctive functional roles, and is described on page 436. The laryngeal cartilages are the single thyroid, cricoid and epiglottic cartilages, and the paired arytenoid, cuneiform, corniculate and tritiate cartilages.
EPIGLOTTIS
The epiglottis is a thin leaf-like plate of elastic fibrocartilage which projects obliquely upwards behind the tongue and hyoid body, and in front of the laryngeal inlet (Figs 34.2, 34.3; see Fig. 34.5). Its free end, which is broad and round, and occasionally notched in the midline, is directed upwards. Its attached part, or stalk (petiolus), is long and narrow and is connected by the elastic thyroepiglottic ligament to the back of the laryngeal prominence of the thyroid cartilage just below the thyroid notch. Its sides are attached to the arytenoid cartilages by aryepiglottic folds (which contain the aryepiglottic muscle). Its free upper anterior, or lingual, surface is covered by mucosa (the epithelium is non-keratinized stratified squamous), which is reflected onto the pharyngeal aspect of the tongue and the lateral pharyngeal walls as a median glossoepiglottic, and two lateral glossoepiglottic, folds. There is a depression, the vallecula, on each side of the median fold. The lower part of its anterior surface, behind the hyoid bone and thyrohyoid membrane, is connected to the upper border of the hyoid by an elastic hyoepiglottic ligament, and separated from the thyrohyoid membrane by adipose tissue, which constitutes the clinically important preepiglottic space. The smooth posterior, or laryngeal, surface is transversely concave and vertically concavo-convex, and is covered by ciliated respiratory mucosa: its lower projecting part is called the tubercle. This surface forms the oblique anterior wall of the laryngeal vestibule. The cartilage is posteriorly pitted by small mucous glands (Fig. 34.3D) and is perforated by branches of the internal laryngeal nerve and fibrous tissue, which means that the posterior surface of the epiglottis is in continuity through these perforations with the pre-epiglottic space.
THYROID CARTILAGE
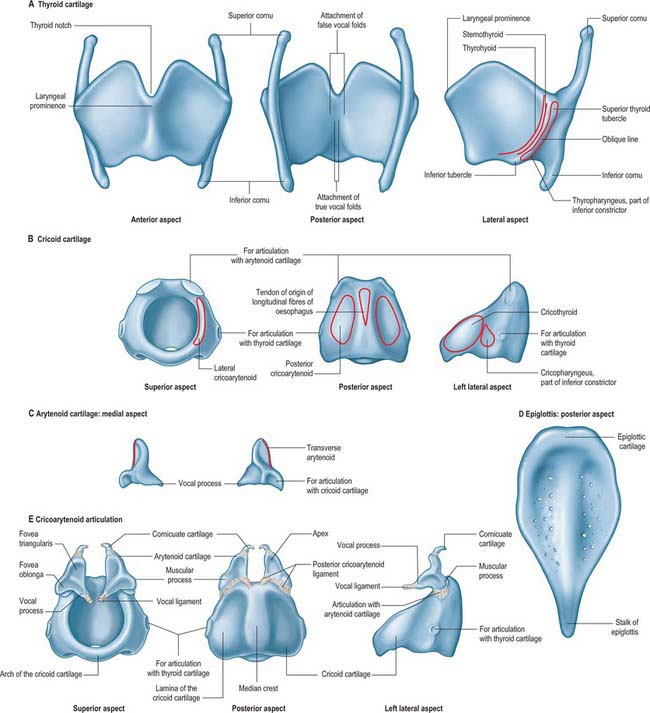
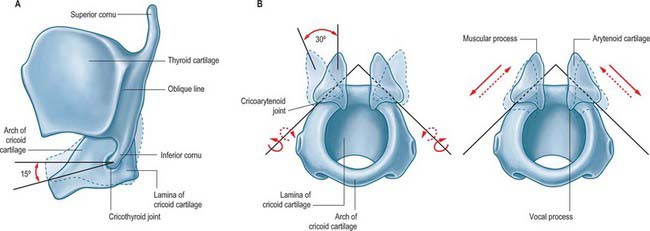
The thyroid cartilage is the largest of the laryngeal cartilages (Figs 34.1–34.3). It consists of two quadrilateral laminae with anterior borders that fuse along their inferior two-thirds at a median angle to form the subcutaneous laryngeal prominence (‘Adam’s apple’). This projection is most distinct at its upper end, and is well marked in men but scarcely visible in women. Above, the laminae are separated by a V-shaped superior thyroid notch or incisure. Posteriorly, the laminae diverge, and their posterior borders are prolonged as slender horns, the superior and inferior cornua. A shallow ridge, the oblique line, curves downwards and forwards on the external surface of each lamina: it runs from the superior thyroid tubercle lying a little anterior to the root of the superior cornu, to the inferior thyroid tubercle on the inferior border of the lamina. Sternothyroid, thyrohyoid and thyropharyngeus (part of the inferior pharyngeal constrictor) are attached to the oblique line, usually as little more than a tendon (Fig. 34.3A).
The internal surface of the lamina is smooth. Above and behind, it is slightly concave and covered by mucosa. The thyroepiglottic ligament, the paired vestibular and vocal ligaments, the thyroarytenoid, thyroepiglottic and vocalis muscles, and the stalk of the epiglottis are all attached to the inner surface of the cartilage, in the angle between the laminae. The true vocal folds lie 6–9 mm below the median thyroid notch. The superior border of each lamina is concave behind and convex in front, and the thyrohyoid membrane is attached along this edge (Figs 34.1, 34.2). The inferior border of each lamina is concave behind and nearly straight in front, and the two parts are separated by the inferior thyroid tubercle. Anteriorly, the thyroid cartilage is connected to the cricoid cartilage by the anterior (median) cricothyroid ligament, which is a thickened portion of the cricothyroid membrane.
CRICOID CARTILAGE
The cricoid cartilage is attached below to the trachea, and articulates with the thyroid cartilage and the two arytenoid cartilages by synovial joints. It forms a complete ring around the airway, the only laryngeal cartilage to do so (Fig. 34.3B). It is smaller, but thicker and stronger, than the thyroid cartilage, and has a narrow curved anterior arch, and a broad, flatter posterior lamina.
Cricoid lamina
A discernible circular synovial facet, facing posterolaterally, sometimes marks the junction of the lamina and arch: it indicates the site where the cricoid articulates with the inferior thyroid cornu. The inferior border of the cricoid is horizontal, and joined to the first tracheal cartilage by the cricotracheal ligament (Fig. 34.1). The superior border runs obliquely up and back, and gives attachment anteriorly to the thick median part of the cricothyroid membrane, and laterally to the membranous parts of the cricothyroid membrane (Fig. 34.1) and lateral cricoarytenoid. The posterosuperior aspect of the lamina presents a shallow median notch, on each side of which is a smooth, oval, convex facet, directed upwards and laterally, for articulation with the base of an arytenoid cartilage.
The internal surface of the cricoid cartilage is smooth and lined by mucosa.
ARYTENOID CARTILAGE
The paired arytenoid cartilages articulate with the lateral parts of the superior border of the cricoid lamina (Figs 34.2, 34.3). Each is pyramidal, and has three surfaces, two processes, a base and an apex. The posterior surface, which is triangular, smooth and concave, is covered by transverse arytenoid. The anterolateral surface is convex and rough, and bears, near the apex of the cartilage, an elevation from which a crest curves back, down and then forwards to the vocal process. The lower part of this arcuate crest separates two depressions (foveae). The upper is triangular (fovea triangularis), and the vestibular ligament is attached to it. The lower is oblong (fovea oblonga), and vocalis and lateral cricoarytenoid are attached to it. The medial surface is narrow, smooth and flat, and is covered by mucosa: its lower edge forms the lateral boundary of the intercartilaginous part of the rima glottidis. The base is concave, with a smooth surface for articulation with the lateral part of the upper border of the cricoid lamina. Its round, prominent lateral angle, or muscular process, projects backwards and laterally: it gives attachment to posterior cricoarytenoid behind, and lateral cricoarytenoid in front. The vocal ligament is attached to its pointed anterior angle (vocal process), which projects horizontally forward. The apex curves backwards and medially and articulates with the corniculate cartilage.
CORNICULATE CARTILAGES
The corniculate cartilages are two conical nodules of elastic fibrocartilage which articulate with the apices of the arytenoid cartilages, prolonging them posteromedially (Fig. 34.3E). They lie in the posterior parts of the aryepiglottic mucosal folds, and are sometimes fused with the arytenoid cartilages.
CUNEIFORM CARTILAGES
The cuneiform cartilages are two small, elongated, club-like nodules of elastic fibrocartilage, one in each aryepiglottic fold anterosuperior to the corniculate cartilages, and are visible as whitish elevations through the mucosa (see Fig. 34.5).
TRITIATE CARTILAGES (CARTILAGO TRITICEA)
The tritiate cartilages are two small nodules of elastic cartilage, situated one on either side above the larynx within the posterior free edge of the thyrohyoid membrane, about halfway between the superior cornu of the thyroid cartilage and the tip of the greater cornu of the hyoid bone (Figs 34.1, 34.2). Their functions are unknown, although they may serve to strengthen this connection.
CALCIFICATION OF LARYNGEAL CARTILAGES
The thyroid, cricoid, and most of the arytenoid cartilages consist of hyaline cartilage, and may therefore become calcified. This process normally starts at about 18 years of age. Initially it involves the lower and posterior part of the thyroid cartilage, and subsequently spreads to involve the remaining cartilages, calcification of the arytenoid cartilage starting at its base. The degree and frequency of calcification of the thyroid and cricoid cartilages appear to be less in females. There is some evidence to suggest that a predilection for tumour invasion may be enhanced by calcification of the laryngeal cartilages.
JOINTS
CRICOTHYROID JOINT
The joints between the inferior cornua of the thyroid cartilage and the sides of the cricoid cartilage are synovial. Each is enveloped by a capsular ligament strengthened posteriorly by fibrous bands (Figs 34.1, 34.2, 34.4). Both capsule and ligaments are rich in elastin fibres. The primary movement at the joint is rotation around a transverse axis which passes transversely through both cricothyroid joints. The effect of this rotation is to move the cricoid and thyroid cartilages relative to one another in such a way as to bring together the lamina of the thyroid cartilage and the arch of the cricoid cartilage (‘closing the visor’). There is some controversy as to which cartilage moves, but it seems most likely that the cricoid cartilage rotates to a greater extent. When the joint is in a neutral position, the ligaments are slack and the cricoid can glide, to a limited extent, in different directions on the thyroid cornua. The effect of these movements is to lengthen the vocal folds, provided the arytenoid cartilages are stabilized at the cricoarytenoid joint. This may also increase vocal fold tension.
CRICOARYTENOID JOINT
The cricoarytenoid joints are a pair of synovial joints between the facets on the lateral parts of the upper border of the lamina of the cricoid cartilage and the bases of the arytenoids. Each joint is enclosed by a capsular ligament and strengthened by a ligament that, although traditionally called the posterior cricoarytenoid ligament, is largely medial in position (Figs 34.1–34.4).
ARYTENOCORNICULATE JOINTS
Synovial or cartilaginous joints link the arytenoid and corniculate cartilages.
SOFT TISSUES
EXTRINSIC LIGAMENTS AND MEMBRANES
Thyrohyoid membrane
The thyrohyoid membrane is a broad, fibroelastic layer attached below to the superior border of the thyroid cartilage lamina and the front of its superior cornua, and above to the superior margin of the body and greater cornua of the hyoid (Figs 34.1, 34.2, 34.5). It thus ascends behind the concave posterior surface of the hyoid, separated from its body by a bursa which facilitates the ascent of the larynx during swallowing. Its thicker part is the median thyrohyoid ligament. The more lateral, thinner, parts are pierced by the superior laryngeal vessels and internal laryngeal nerves (Fig. 34.1). Externally, it is in contact with thyrohyoid and omohyoid and the body of the hyoid bone. Its inner surface is related to the lingual surface of the epiglottis and the piriform fossae of the pharynx. The round, cord-like, elastic lateral thyrohyoid ligaments form the posterior borders of the thyrohyoid membrane, and connect the tips of the superior thyroid cornua to the posterior ends of the greater hyoid cornua (Fig. 34.1).
INTRINSIC LIGAMENTS AND MEMBRANES
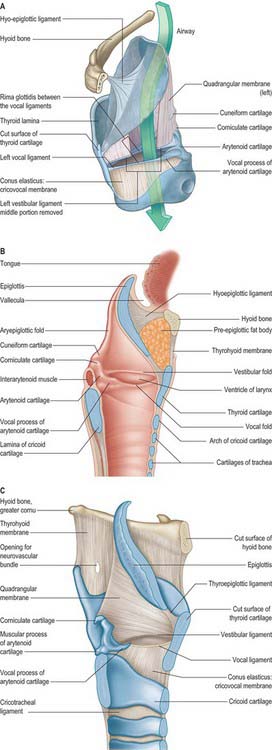
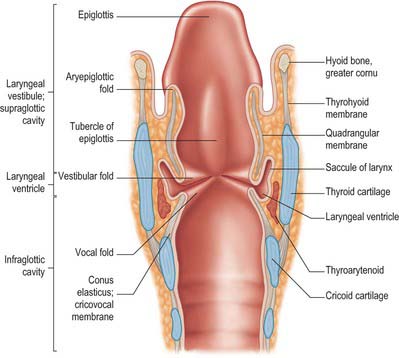
The fibroelastic membrane of the larynx lies within the cartilaginous skeleton of the larynx, beneath the laryngeal mucosa (Fig. 34.5). It forms a discontinuous sheet separated on both sides of the larynx by a horizontal cleft between the vestibular and vocal ligaments. Its upper part, the quadrangular membrane, extends between the arytenoid cartilages and the sides of the epiglottis. Its lower part, the cricothyroid membrane and conus elasticus, connects the thyroid, cricoid and arytenoid cartilages.
LARYNGEAL CAVITY
The laryngeal cavity extends from the laryngeal inlet (from the pharynx) down to the lower border of the cricoid cartilage, where it continues into the trachea (Figs 34.5, 34.6). The walls of the cavity are formed of the fibroelastic membranes described above and are lined with mucous membrane which folds over the free edges of these fibroelastic membranes within the larynx. On either side, the continuity of the fibroelastic membrane is interrupted between the upper and lower folds.
MICROSTRUCTURE OF THE LARYNX
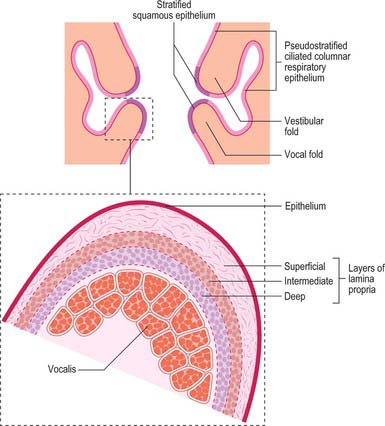
The laryngeal epithelium is mainly a ciliated, pseudostratified respiratory epithelium where it covers the inner aspects of the larynx, including the posterior, laryngeal surface of the epiglottis, and it provides a mucociliary clearance mechanism shared with most of the respiratory tract (see Ch. 57). However, the vocal folds are covered by non-keratinized, stratified squamous epithelium where they contact each other: this important variation protects the tissue from the effects of the considerable mechanical stresses that act on the surfaces of the vocal folds. The exterior surfaces of the larynx, which merge with the laryngopharynx and oropharynx (including the anterior, lingual surface of the epiglottis and the aryepiglottic folds), are subject to the abrasive effects of swallowed food, and are therefore covered by non-keratinized, stratified squamous epithelium.
UPPER PART
Aryepiglottic fold
The aryepiglottic fold contains ligamentous and muscular fibres. The ligamentous fibres represent the free upper border of the quadrangular membrane (Fig. 34.5). The muscle fibres are continuations of the oblique arytenoids. The posterior part of the aryepiglottic fold contains two oval swellings, one above and in front, the other behind and below, that mark the positions of the underlying cuneiform and corniculate cartilages respectively. They are separated by a shallow vertical furrow which is continuous below with the opening of the laryngeal ventricle.
MIDDLE PART
Vestibular folds and ligaments
The narrow vestibular ligament represents the thickened lower border of the quadrangular membrane (Fig. 34.5). It is fixed in front to the thyroid angle below the epiglottic cartilage and behind to the anterolateral surface of the arytenoid cartilage above its vocal process. With its covering of mucosa, it is termed the vestibular (ventricular or false vocal) fold (Figs 34.5, 34.6). The presence of a loose vascular mucosa lends the vestibular folds a pink appearance in vivo, as they lie above and lateral to the vocal cords.
Ventricle (sinus) of the larynx
The laryngeal ventricle is a slit between the vestibular and vocal cords (Figs 34.5, 34.6). It opens into a fusiform recess on each side of the larynx and extends upwards into the laryngeal wall lateral to the vestibular fold, opening into the saccule.
Saccule of the larynx
The saccule is a pouch which ascends forwards from the ventricle, between the vestibular fold and thyroid cartilage, and occasionally reaches the upper border of the cartilage (Fig. 34.6). It is conical, and curves slightly backwards; 60–70 mucous glands, sited in the submucosa, open onto its luminal surface. The orifice of the saccule is guarded by a delicate fold of mucosa, the ventriculosaccular fold.
Vocal folds (cords) and ligaments
The free thickened upper edge of the conus elasticus forms the vocal ligament. It stretches back on either side from the mid level of the thyroid angle to the vocal processes of the arytenoids. When covered by mucosa, it is termed the vocal fold or vocal cord (cord is the preferred clinical term) (Figs 34.5, 34.6). The vocal folds form the anterolateral edges of the rima glottidis and are concerned with sound production. Each fold consists of five layers, namely mucosa, lamina propria (three layers) and the vocalis muscle (Fig. 34.7).
Rima glottidis
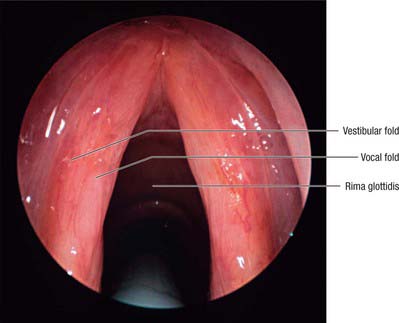
The rima glottidis or glottis is the fissure between the vocal cords anteriorly and the arytenoid cartilages posteriorly (see Figs 34.8, 34.9). It is bounded behind by the mucosa that passes between the arytenoid cartilages at the level of the vocal cords. The glottis is customarily divided into two regions, an anterior intermembranous part, which makes up about three-fifths of its anteroposterior length and is formed by the underlying vocal ligament, and a posterior intercartilaginous part formed by the vocal processes of the arytenoid cartilages. It is the narrowest part of the larynx, having an average sagittal diameter in adult males of 23 mm, and in adult females of 17 mm: its width and shape vary with the movements of the vocal cords and arytenoid cartilages during respiration and phonation (see p. 590).
LARYNGOSCOPIC EXAMINATION
The laryngeal inlet, the structures around it, and the cavity of the larynx can all be inspected using fibreoptic endoscopy, through either the mouth or nasopharynx. The epiglottis is seen foreshortened, but its tubercle is visible. From the epiglottic margins the aryepiglottic folds can be traced posteromedially and the cuneiform and corniculate elevations recognized. The pink vestibular folds and pearly white vocal cords are visible and, when the rima glottidis is wide open, the anterior arch of the cricoid cartilage, the tracheal mucosa and cartilages may be seen (Fig. 34.8). The piriform fossae can also be inspected.
THE INFANT LARYNX
The infant larynx differs markedly from its adult counterpart. Although it is about one-third adult size, it is proportionately larger. Its lumen is short and funnel-shaped and disproportionately narrower than that of the adult. It lies higher in the neck than the adult larynx (see Fig. 33.10). At rest, the upper border of the infant epiglottis is at the level of the second or third cervical vertebra; when the larynx is elevated, it reaches the level of the first cervical vertebra. This high position enables an infant to use its nasal airway to breathe while suckling. The epiglottis is X-shaped, with a furled petiole, and the laryngeal cartilages are softer and more pliable than in the adult larynx (which may predispose to airway collapse in inspiration, leading to the clinical picture of laryngomalacia). The thyroid cartilage is shorter and broader and lies closer to the hyoid bone in the neonate, which means that the thyrohyoid ligament is relatively short. Neither the superior notch nor the laryngeal prominence are as marked as they are in the adult. The cricoid cartilage is the same shape as in the adult. The arytenoid cartilages are more prominent and the aryepiglottic folds are disproportionally large. The vocal cords are 4–4.5 mm long, which is relatively shorter than in either childhood or the adult. The ventricle of the larynx is small, whereas the saccule of the larynx is often considerably larger than it is in adult life.
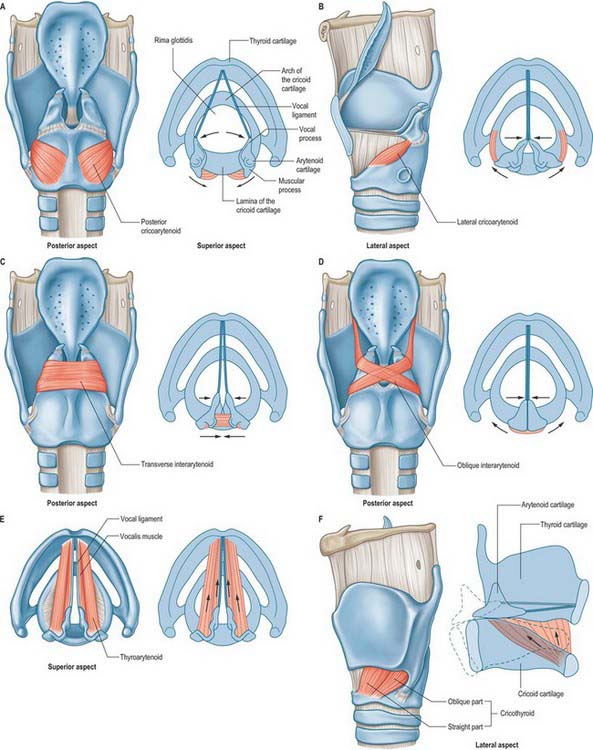
MUSCLES
The intrinsic muscles are the cricothyroid, posterior and lateral cricoarytenoid, transverse and oblique arytenoid, aryepiglotticus, thyroarytenoid and its subsidiary part, vocalis, and thyroepiglotticus: all are confined to the larynx in their attachments, and all but the transverse arytenoid are paired (Fig. 34.9). Whereas most of the intrinsic muscles lie internally, under cover of the thyroid cartilage or the mucosa, the cricothyroids appear on the outer aspect of the larynx.
INTRINSIC MUSCLES
Transverse (inter) arytenoid
Transverse arytenoid is a single, unpaired muscle deep to the oblique interarytenoids (Fig. 34.9C). It bridges the gap at the back of the larynx between the two arytenoid cartilages and fills their posterior concave surfaces. It is attached to the back of the muscular process and adjacent lateral border of both arytenoids.
Transverse arytenoid pulls the arytenoid cartilages towards each other, closing the posterior, intercartilaginous, part of the rima glottidis, such as occurs during a whisper (Fig. 34.9C). This action is accomplished by drawing the arytenoids upwards to slide along the sloping shoulders of the cricoid lamina, without rotation.
Posterior cricoarytenoid
Posterior cricoarytenoid arises from the posterior surface of the cricoid lamina (Fig. 34.9A). Its fibres ascend laterally and converge to insert on the upper and posterior surfaces of the muscular process of the ipsilateral arytenoid cartilage. The highest fibres run almost horizontally, the middle obliquely, and the lowest are almost vertical: some reach the anterolateral surface of the arytenoid cartilage. An additional strip of muscle, ceratocricoid, is occasionally seen in relation to the lower border of posterior cricoarytenoid, arising from the cricoid cartilage and inserting onto the posterior aspect of the inferior cornu of the thyroid cartilage.
The posterior cricoarytenoids are the only laryngeal muscles that open the glottis. They rotate the arytenoid cartilages laterally around an axis that passes through the cricoarytenoid joints, producing separation of the vocal processes and the attached vocal cords (Fig. 34.9A). They also pull the arytenoids backwards, assisting the cricothyroids to lengthen the vocal cords. The most lateral fibres draw the arytenoid cartilages laterally, and so the rima glottidis becomes triangular when the posterior cricoarytenoid muscles contract. The posterior cricoarytenoids are active in the production of unvoiced sounds.
Lateral cricoarytenoid
Lateral cricoarytenoid is attached anteriorly to the upper border of the cricoid arch. It ascends obliquely backwards to be attached to the front of the muscular process of the ipsilateral arytenoid cartilage (Fig. 34.9B).
Lateral cricoarytenoid rotates the arytenoid cartilage in a direction opposite to that of posterior cricoarytenoid, and so closes the rima glottidis (Fig. 34.9B). As it does so, it brings the tips of the vocal processes together, closing the ligamentous part of the rima glottidis, an action known as medial compression. The action of lateral cricoarytenoid in adducting the vocal folds is therefore distinct and complementary to that of the interarytenoid muscles. Contraction of lateral cricoarytenoid also results in shortening and relaxing of the vocal folds.
Cricothyroid
Cricothyroid is attached anteriorly to the external aspect of the arch of the cricoid cartilage (Fig. 34.9F). Its fibres pass backwards and diverge into two groups, a lower ‘oblique’ part which slants backwards and laterally to the anterior border of the inferior cornu of the thyroid, and a superior ‘straight’ part which ascends more steeply backwards to the posterior part of the lower border of the thyroid lamina. The medial borders of the paired cricothyroids are separated anteriorly by a triangular gap occupied by the median cricothyroid ligament.
Thyroarytenoid and vocalis
Thyroarytenoid is a broad, thin muscle, lying lateral to the vocal fold, conus elasticus, laryngeal ventricle and saccule (Fig. 34.9E). It is attached anteriorly to the lower half of the angle of the thyroid cartilage, and to the cricothyroid ligament. Its fibres pass backwards, laterally and upwards to the anterolateral surface of the arytenoid cartilage. The lower and deeper fibres form a band which, in coronal section, appears as a triangular bundle attached to the lateral surface of the vocal process and to the inferior impression on the anterolateral surface of the arytenoid cartilage. This bundle, the vocalis muscle, is parallel with, and just lateral to, the vocal ligament. It is said to be thicker behind than in front, because many deeper fibres start from the vocal ligament and do not extend to the thyroid cartilage. (An alternative view is that all its fibres loop and intertwine as they pass from the thyroid to the arytenoid cartilage.) A few fibres extend along the wall of the ventricle from the lateral margin of the arytenoid cartilage to the side of the epiglottis. Superior thyroarytenoid, an inconstant small muscle, lies on the lateral surface of the main mass of thyroarytenoid; when present, it extends obliquely from the thyroid angle to the muscular process of the arytenoid cartilage.
VASCULAR SUPPLY AND LYMPHATIC DRAINAGE
The blood supply of the larynx is derived mainly from the superior and inferior laryngeal arteries (Fig. 34.10). Rich anastomoses exist between the corresponding contralateral laryngeal arteries and between the ipsilateral laryngeal arteries. The superior laryngeal arteries supply the greater part of the tissues of the larynx, from the epiglottis down to the level of the vocal cords, including the majority of the laryngeal musculature. The inferior laryngeal artery supplies the region around cricothyroid, while its posterior laryngeal branch supplies the tissue around posterior cricoarytenoid.
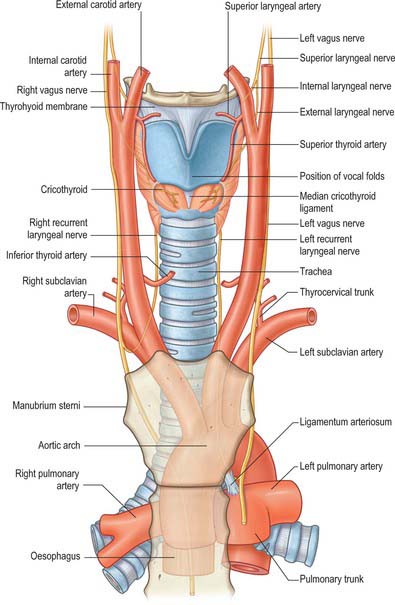
Fig. 34.10 Anterior view of the blood supply and innervation of the larynx.
(From Drake, Vogl and Mitchell 2005.)
INNERVATION
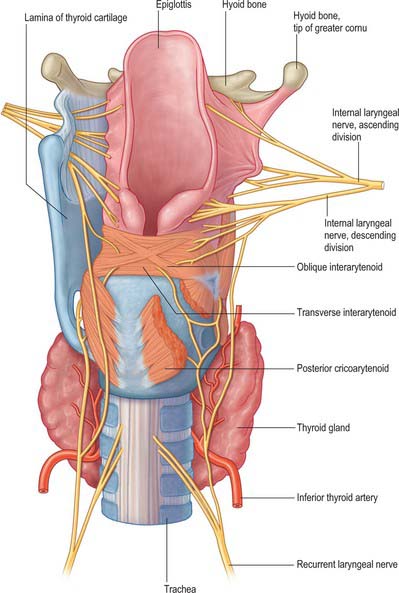
The larynx is innervated by the internal and external branches of the superior laryngeal nerve, the recurrent laryngeal nerve and sympathetic nerves (Figs 34.10, 34.11). Conventionally, the internal laryngeal nerve is described as sensory, the external laryngeal nerve as motor, and the recurrent laryngeal nerve as mixed. The internal laryngeal nerve is sensory down to the vocal cords, the recurrent laryngeal nerve is sensory below the vocal cords, and there is overlap between the territories innervated by the two nerves at the vocal cords themselves. All the intrinsic muscles of the larynx are supplied by the recurrent laryngeal nerve except for cricothyroid, which is supplied by the external laryngeal nerve. However, a number of anastomoses between these three nerves have been described, with varying estimates of their incidence. The majority occur on the posterior surface of the larynx, forming what has been described as a laryngeal plexus to parallel the pharyngeal plexus. Their precise nature and function is unclear, but since some are thought to convey motor fibres, it is reasonable to assume that functions commonly ascribed to the three laryngeal nerves may be more complex than the conventional descriptions imply, and this may have potential clinical implications.
The detailed course of the vagus in the neck is described on page 458.
Superior laryngeal nerve
External laryngeal nerve
The external laryngeal nerve continues downwards and forwards on the lateral surface of the inferior constrictor, to which it contributes some small branches. Indeed, in approximately 30% of cases, the nerve is located within the fibres of the constrictor muscle. It passes beneath the attachment of sternothyroid to the oblique line of the thyroid cartilage and supplies cricothyroid. A communicating nerve continues from the posterior surface of cricothyroid, crosses the piriform fossa and enters thyroarytenoid, where it anastomoses with branches from the recurrent laryngeal nerve. It has been suggested that these communicating branches may provide both additional motor components to thyroarytenoid and sensory fibres to the mucosa in the region of the subglottis. An anastomosis between the external and internal laryngeal nerves has also been described in some cases.
Recurrent laryngeal nerve
The recurrent laryngeal nerve forms several anastomoses with the superior laryngeal nerves (Fig. 34.11). The posterior branch of the recurrent laryngeal nerve ascends deep to posterior cricoarytenoid to join the descending branch of the internal laryngeal nerve. In addition, the ansa Galeni that lies on the interarytenoid muscles forms a direct connection between the recurrent and internal laryngeal nerves (Fig. 34.11), while there is also a complex anastomosis within and over the posterior surface of the interarytenoid muscles; and, less frequently, anastomoses on the cricoid lamina and thyroarytenoid that also form connections with the internal laryngeal nerve.
Outside its capsule the thyroid gland has a distinct covering of pretracheal fascia which splits into two layers at the posterior border of the gland. One layer covers the entire medial surface of its lobe; at, or just above, the isthmus it is conspicuously thickened to form the lateral ligament of the thyroid gland, which attaches the gland to the trachea and the lower part of the cricoid cartilage. The other layer is posterior; it passes behind the oesophagus and pharynx and is attached to the prevertebral fascia (p. 439). In this way, a compartment is formed on each side of the midline, lateral to the trachea and oesophagus: the recurrent laryngeal nerve and terminal parts of the inferior thyroid artery lie in the fat of this compartment. The nerve may be lateral or medial to the lateral ligament of the thyroid gland, and sometimes may be embedded in it.
An very rare anomaly that is of relevance to laryngeal pathology and surgery is the so-called ‘non-recurrent’ laryngeal nerve, where the right recurrent laryngeal nerve arises directly from the vagus nerve trunk high up in the neck and enters the larynx close to the inferior pole of the thyroid gland. Only the right side is affected, and it is always associated with an abnormal origin of the right subclavian artery from the aortic arch on the left side. If unrecognized, a non-recurrent laryngeal nerve may be susceptible to injury during surgery. It may also potentially be compressed by small tumours of the thyroid gland (p. 462).
ANATOMY OF SPEECH
The principal biological function of the larynx is to act as a sphincter controlling the entry of foreign bodies into the airways and regulate airflow during ventilation. Thus, the larynx is opened widely during ventilation and is closed tightly during swallowing. The larynx can also close tightly during exertion, effort closure, to regulate thoracic and abdominal pressure during activities such as defecation or parturition, or to fix the thorax to increase mechanical advantage when using the arms to lift objects. The importance of the latter activity should not be underestimated: one of the many problems reported by patients who have undergone a laryngectomy is a loss of power in their arms when trying to lift heavy objects.
MUSCULAR CONTROL OF THE AIRSTREAM
The non-rhythmical pattern during speech requires greater inspiratory effort, and for most people it involves a greater use of the diaphragm, usually in combination with the abdominal muscles that are attached to the lower ribs (they stabilize the costal attachments of the diaphragm and increase the effectiveness of its action) (see p. 1011). However, the main differences are seen in expiration. Speech takes place at higher lung volumes, which means that greater recoil forces are stored in the elastic tissues of the lungs and the ribcage. The generation of subglottal pressure is the product of these elastic recoil forces and the muscular forces generated by the expiratory muscles. At the onset of an utterance, unrestrained recoil forces would generate excessive subglottal pressures that would be wasteful of air, and hence energy, and would affect the loudness of speech. Conversely, towards the end of an utterance, as recoil forces decline, subglottal pressure would fall without additional muscular exertion. Therefore, early in an utterance, inspiratory muscles, particularly the external intercostals and parasternal parts of the internal intercostals, continue to contract, relaxing slowly to counteract the effects of excessive passive elastic recoil. As the recoil forces decline below the point where they can maintain the minimum subglottal pressure needed for phonation, expiratory muscles contract to maintain subglottal pressure as lung air volume nears its resting expiratory level. The main muscles involved are the costal parts of the internal intercostals and the subcostal and transversus thoracis muscles. Their actions are aided by contraction of the anterior abdominal muscles to compress the abdomen. Accessory muscles such as latissimus dorsi may also come into play, but normally these accessory muscles are only active at the end of a very long or loud utterance, or in patients whose ventilatory function is compromised.
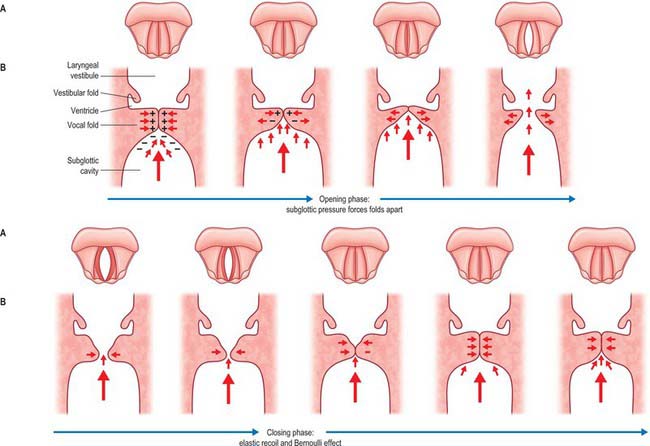
PHONATION
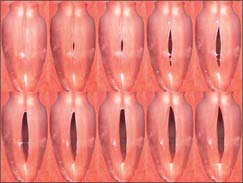
The default position of the rima glottidis is open, to maintain patency of the airway during respiration. In quiet respiration, the anterior intermembranous part of the rima glottidis is triangular when viewed from above. Its apex is anterior and its base posterior, and it is represented by an imaginary line approximately 8 mm long connecting the anterior ends of the arytenoid vocal processes. The intercartilaginous part between the medial surfaces of the arytenoids is rectangular as the two vocal processes lie parallel to each other. During forced respiration, the rima glottidis is widened and the vocal cords are fully abducted to increase the airway. The arytenoid cartilages rotate laterally, and this moves their vocal processes apart, and converts the rima glottidis into a diamond shape in which both intermembranous and intercartilaginous parts are triangular. The greatest width of the rima glottidis is at the point of the attachments of the vocal cords to the vocal processes.
At the onset of an utterance, during an expiration, the true vocal folds are adducted: the lateral cricoarytenoids and interarytenoids bring together both the intermembranous and intercartilaginous parts of the glottis, actions which either close the glottis completely or reduce the space between the vocal folds to a linear chink. The mucous membrane covering the interarytenoid muscles, the interarytenoid fold, intrudes into the larynx when these muscles adduct the arytenoids, and so aids closure of the intercartilaginous part of the rima glottidis. The vocal cords are also tensed, an essential prerequisite for vibration. These actions cause a build-up of subglottal pressure that continues until a point is reached when the muscular force of adduction is no longer sufficient to resist the rising pressure, and the vocal folds are forced open a little, releasing air into the supralaryngeal vocal tract. The subglottal pressure falls when the subglottic and supraglottic cavities become continuous and the vocal folds begin to close. Two mechanisms bring about closure. If adductive tension is sustained, then the vocal folds will close. In addition, rapid closure is aided by a physical process, the Bernoulli effect. The forcing of air from a region of high to low pressure through a narrow space causes an increase in the kinetic energy of the molecules at the edge of the space. The effect of this is to lower pressure in the space between the folds at the level of the folds themselves, and this negative pressure simply sucks the folds together because they are mobile. This causes a rise once more in the subglottal pressure and the cycle is repeated. The effect is to cause the release of a series of puffs of air into the supralaryngeal vocal tract at a frequency of many times per second, which is perceived as a sound of a particular frequency (Figs 34.12, 34.13).
The aerodynamic–myoelastic theory does not explain how vocal fold vibration is sustained, nor does it account for the very obvious muco-undulatory component of vocal fold vibration that is visible when the larynx is viewed stroboscopically. Without further input of energy the vibration of the vocal folds as described above would not be sustained but would be damped and gradually diminish. For vibration to continue there has to be additional energy input. The analogy here is with a child on a swing. For the motion to continue either the parent has to push the child at an appropriate point in the cycle, or the child has to sustain the motion for themselves by swinging their legs at the crucial point in the swing cycle. In the case of phonation, the source of this additional energy is unclear. It may come from the inertia of the air column itself, i.e. once the vocal folds close, the air column will continue moving upwards because inertia creates a negative pressure above the folds. Alternatively, the energy could come from the manner in which the folds open and close. As the subglottal pressure rises, the lower portion of the fold opens first and the upper edge of the fold is last to open, and when the subglottal pressure falls, the folds close from the bottom edge. It has been suggested that this non-uniform closure creates different shapes within the glottis that may result in differing negative pressures at different phases of the cycle. It also produces a vertical wave-like motion in the folds, termed the muco-undulatory component. The analogy here is with a flag blowing in the wind, and it reflects the differing stiffnesses of the various layers of the vocal folds described above. This vertical component will impart a negligible amount of energy to the air column, but it is likely to impart harmonics to the basic laryngeal vibration.
ARTICULATION
The human vocal tract can produce many more phonemes than are employed in any one language. Not all languages have the same phonemes, and within the same language, the phonemes can vary in different parts of the same country and in other countries where that language is also spoken. Reproducing phonemes that are not used in native speech is difficult because such phonemes require unfamiliar positioning of the speech organs. A native speaker of any language can quickly recognize the origins of anyone attempting to use their language as a second language. The second-language speaker will usually speak it with an accent characteristic of their own first language because they are using the familiar configurations of their vocal tract for each phoneme instead of the correct positioning.
PRODUCTION OF CONSONANTS
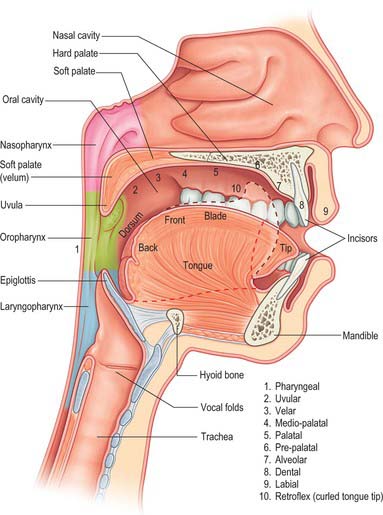
Consonants may also be classified as labial, dental, alveolar, velar, uvular, pharyngeal or glottic, depending upon whether the point of maximum constriction occurs at the level of the lips, teeth, bony ridge behind the teeth, palate, uvula or pharynx (Fig. 34.14). Different parts of the tongue can be used in combination with the above places of articulation. Phoneticians divide the tongue into the tip, anterior edge, the front part of the dorsum, the centre and back parts of the remaining dorsum, and a most posterior part (the root). These divisions bear no obvious relationship to the anatomical landmarks on the tongue, but they are useful in describing the part of the dorsum of the tongue that contacts other areas of the mouth. Similarly, the manner of articulation can vary from a complete closure to a slight narrowing. An actual closure of the vocal tract is called a stop. A narrowing that is sufficient to produce turbulence of the air in the vocal tract, and which is perceived as a rustling sound, is termed a fricative. Approximants involve a degree of closure insufficient to produce turbulence but with closure greater than that for a vowel. Nasals involve a stoppage in the oral cavity with the soft palate lowered to allow airflow through the nose, and, unlike stops, they can be sustained. Stricture describes the shape of the constriction, e.g. a lateral consonant involves depression of the sides of the tongue, while a grooved consonant is produced by grooving the dorsum of the tongue. Consonants can be produced with the vocal folds vibrating, when they are termed voiced, or without vocal fold vibration, in which case they are termed unvoiced.
Atkinson M, McHanwell S. Basic Medical Science for Speech & Language Therapy Students. London: Whurr Publishers, 2002.
Berkovitz BKB, Moxham BJ, Hickey S. The anatomy of the larynx. In: Ferlito A, editor. Diseases of the Larynx. London: Chapman & Hall; 2000:25-44.
Bosma JF, Bartner MA. Ligaments of the larynx and the adjacent pharynx and esophagus. Dysphagia. 1993;8:23-28.
Clark J, Yallop C. An Introduction to Phonetics and Phonology, 2nd edn. Oxford: Blackwell, 1995.
A comprehensive introduction to all aspects of phonetics and phonology..
Durham FC, Harrison TS. The surgical anatomy of the superior laryngeal nerve. Surg Gynecol Obstet. 1962;118:33-44.
Erkki A, Pitkanen R, Suominen H. Observations on the structure and the biomechanics of the cricothyroid articulation. Acta Otolaryngol (Stockh). 1987;103:117-126.
Friedman M, Toriumi DM, Grybauskas V, Katz A. Nonrecurrent laryngeal nerves and their clinical significance. Laryngoscope. 1986;96:87-90.
Kirchner JA, Carter D. Intralaryngeal barriers to the spread of cancer. Acta Otolaryngol (Stockh). 1987;103:503-513.
Maranillo E, Leon X, Orus C, Quer M, Sanudo J-R. Variability in nerve patterns of the adductor muscle group supplied by the recurrent laryngeal nerve. Laryngoscope. 2005;115:358-362.
Munir Turk L, Hogg DA. Age changes in the human laryngeal cartilages. Clin Anat. 1993;6:154-162.
Pracy R. The infant larynx. J Laryngol Otol. 1983;97:933-947.
Reidenbach MM. Normal topography of the conus elasticus. Anatomical bases for the spread of laryngeal cancer. Surg Radiol Anat. 1995;17:107-111.
Reidenbach MM. The periepiglottic space: topographic relations and histological organisation. J Anat. 1996;188:173-182.
Reidenbach MM. The paraglottic space and transglottic cancer: anatomic considerations. Clin Anat. 1996;9:244-251.
Reidenbach MM. Subglottic region: normal topography and possible clinical implications. Clin Anat. 1998;11:9-21.
Sanudo J-R, Maranillo E, León X, Mirapeix R-M, Orús C, Quer M. An anatomical study of anastomoses between the laryngeal nerves. Laryngoscope. 1999;109:983-987.
Sato I, Shimada K. Arborization of the inferior laryngeal nerve and internal nerve on the posterior surface of the larynx. Clin Anat. 1995;8:379-387.
Welsh LW, Welsh JJ, Rizzo TA. Laryngeal spaces and lymphatics: current anatomic concepts. Ann Otol Rhinol Laryngol Suppl. 1983;105:19-31.






