Chapter 4 Laparoscopic Repair of Parastomal Hernias 
1 Clinical Anatomy
1 Types of Parastomal Hernias
Parastomal hernia has been anatomically classified into four subtypes: (Fig. 4-1)



2 Preoperative Considerations
 The life expectancy of the patient and any predisposing factors, such as malignancy and obesity, should influence the decision to proceed with surgery.
The life expectancy of the patient and any predisposing factors, such as malignancy and obesity, should influence the decision to proceed with surgery.






3 Operative Steps
There are two techniques for laparoscopic repairs of parastomal hernias: the keyhole and the Sugarbaker techniques. Keyhole technique may be associated with bowel herniation between the mesh hole and the stoma loop. We have developed a technique that closes the gap between the mesh and the stoma loop and facilitates intracorporeal mesh manipulations (Scroll technique) during keyhole repairs. The Sugarbaker technique avoids the risk of herniation through the keyhole, but it does create an acute angle as the bowel exits the mesh and can cause obstruction (see Fig. 4-11). Meticulous attention to the details of mesh fixation and placement can limit these complications.
 1 Laparoscopic Parastomal Hernia Repair Technique: The Scroll Technique
1 Laparoscopic Parastomal Hernia Repair Technique: The Scroll Technique






 Trocar Placement (Fig. 4-4)
Trocar Placement (Fig. 4-4)





 Lysis of Adhesions
Lysis of Adhesions
 Lysis of adhesions is the most challenging part of this procedure; this is performed using sharp or blunt dissection as close as possible to the anterior abdominal wall.
Lysis of adhesions is the most challenging part of this procedure; this is performed using sharp or blunt dissection as close as possible to the anterior abdominal wall.



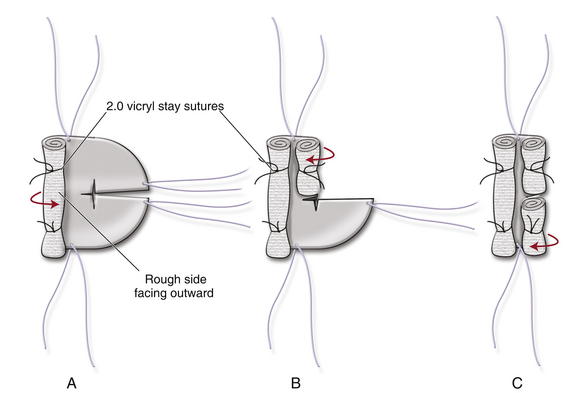
 Mesh Choice and Preparation (Figs. 4-5 and 4-6)
Mesh Choice and Preparation (Figs. 4-5 and 4-6)

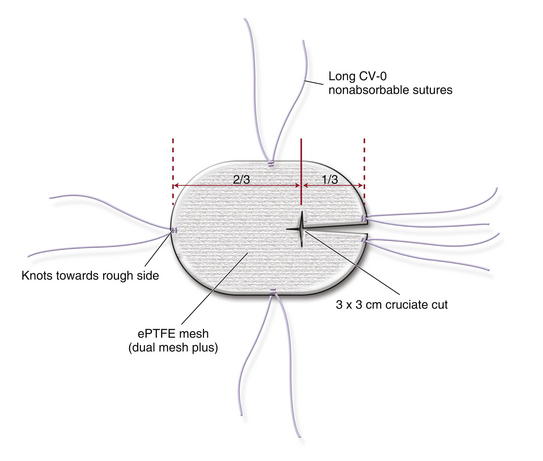
 Keyhole Technique
Keyhole Technique
 The mesh is fashioned by creating a 3 × 3 cm cruciate cut at the junction of two thirds and one third of the mesh (see Fig. 4-5).
The mesh is fashioned by creating a 3 × 3 cm cruciate cut at the junction of two thirds and one third of the mesh (see Fig. 4-5).




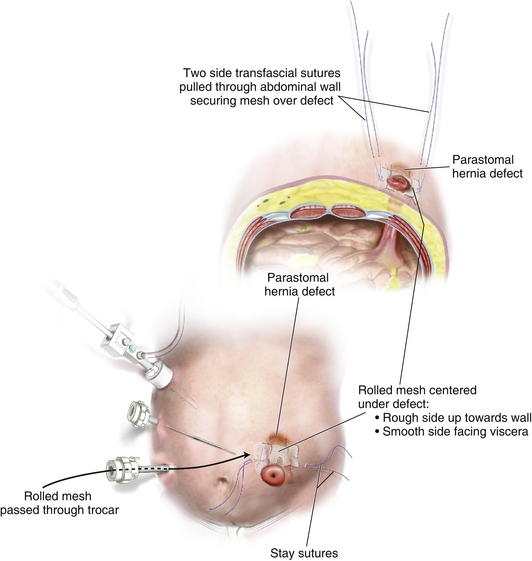
 Mesh Fixation
Mesh Fixation
 Once the mesh is inside the abdominal cavity, the two transfascial sutures at the sides of the mesh are pulled through the abdominal wall with the suture passer. This will bring the rolled mesh adherent to the abdominal wall, centering it over the defect with the mesh split toward the colostomy side (Fig. 4-7).
Once the mesh is inside the abdominal cavity, the two transfascial sutures at the sides of the mesh are pulled through the abdominal wall with the suture passer. This will bring the rolled mesh adherent to the abdominal wall, centering it over the defect with the mesh split toward the colostomy side (Fig. 4-7).
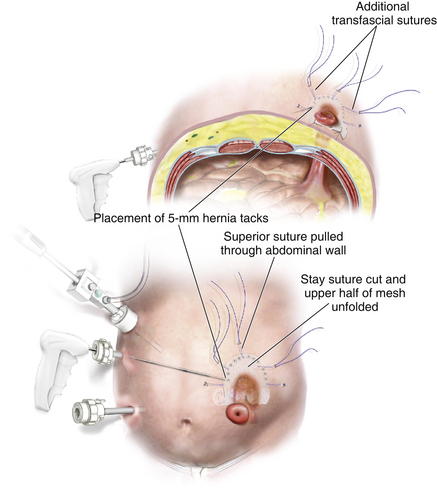
 The transabdominal sutures are tied. The Vicryl stay suture is cut, and the upper half of the mesh is unfolded (Fig. 4-8).
The transabdominal sutures are tied. The Vicryl stay suture is cut, and the upper half of the mesh is unfolded (Fig. 4-8).
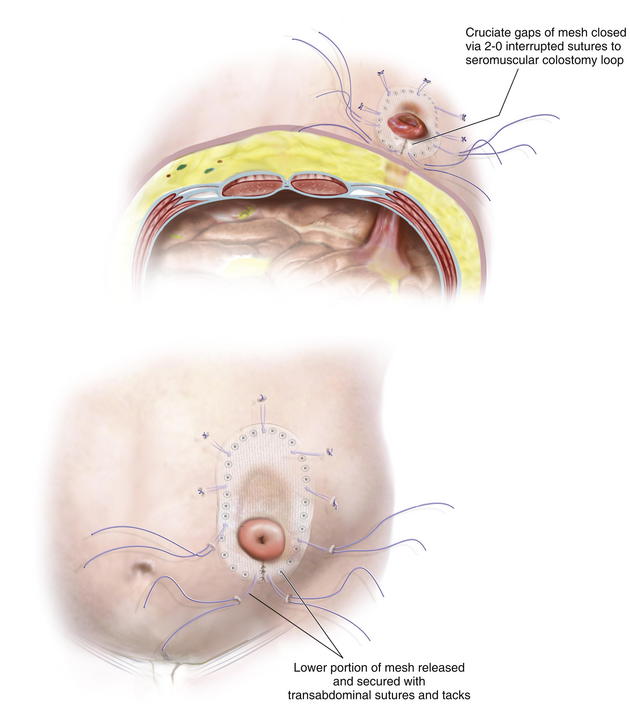
 Next, 5-mm hernia tacks are placed circumferentially, 1 cm from the edge of the mesh and 1 to 2 cm apart.
Next, 5-mm hernia tacks are placed circumferentially, 1 cm from the edge of the mesh and 1 to 2 cm apart. The same procedure is repeated on the other half of the mesh (Fig. 4-9), cutting the Vicryl stay suture and spreading each part of the lower portion of the mesh individually. The mesh portions are fixed using transabdominal sutures and 5-mm hernia tacks.
The same procedure is repeated on the other half of the mesh (Fig. 4-9), cutting the Vicryl stay suture and spreading each part of the lower portion of the mesh individually. The mesh portions are fixed using transabdominal sutures and 5-mm hernia tacks.




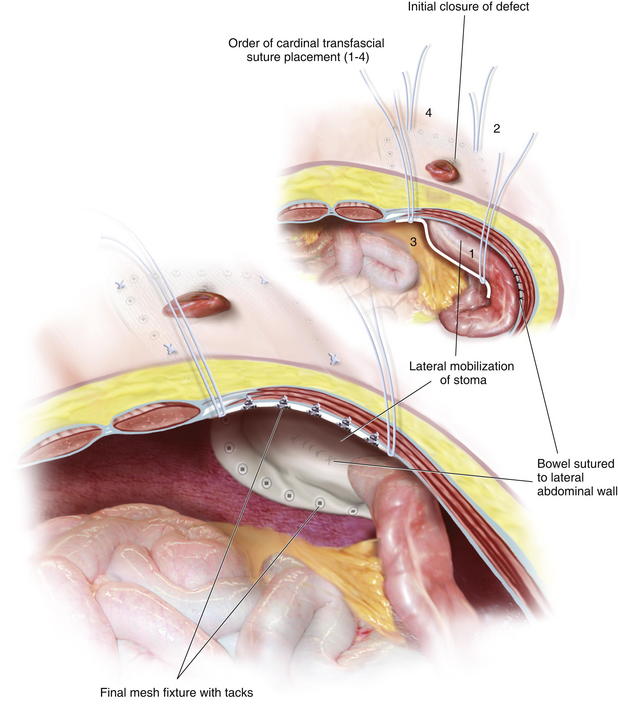
 2 Laparoscopic Sugarbaker Technique (Fig. 4-11)
2 Laparoscopic Sugarbaker Technique (Fig. 4-11)
 The laparoscopic Sugarbaker technique involves placing a flat sheet of mesh on the abdominal wall and lateralizing the stoma’s loop of bowel. In order to perform this procedure, the bowel must have sufficient mobilization to allow it to be displaced laterally without excessive kinking. Occasionally, ileal conduit hernias cannot be lateralized because of the posterior fixation of the ureters.
The laparoscopic Sugarbaker technique involves placing a flat sheet of mesh on the abdominal wall and lateralizing the stoma’s loop of bowel. In order to perform this procedure, the bowel must have sufficient mobilization to allow it to be displaced laterally without excessive kinking. Occasionally, ileal conduit hernias cannot be lateralized because of the posterior fixation of the ureters.











5 Pearls/Pitfalls









Berger D., Bientzle M. Laparoscopic repair of parastomal hernias: a single surgeon’s experience in 66 patients. Dis Colon Rectum. 2007 Oct;50(10):1668-1673.
Craft R.O., Huguet K.L., McLemore E.C., Harold K.L. Laparoscopic parastomal hernia repair. Hernia. 2008 Apr;12(2):137-140.
Hansson B.M., Bleichrodt R.P., de Hingh I.H. Laparoscopic parastomal hernia repair using a keyhole technique results in a high recurrence rate. Surg Endosc. 2009 Jul;23(7):1456-1459.
Muysoms E.E., Hauters P.J., Van Nieuwenhove Y., Huten N., Claeys D.A. Laparoscopic repair of parastomal hernias: a multi-centre retrospective review and shift in technique. Acta Chir Belg. 2008 Jul-Aug;108(4):400-404.
Muysoms F. Laparoscopic repair of parastomal hernias with a modified Sugarbaker technique. Acta Chir Belg. 2007 Jul-Aug;107(4):476-480.
Saber A.A., Rao A.J., Rao C.A., Elgamal M.H. Simplified laparoscopic parastomal hernia repair: the scroll technique. Am J Surg. 2008 Sep;196(3):16-18.
