CHAPTER ELEVEN KNEE
INTRODUCTION
Pain is the most common presenting symptom of knee abnormalities. The causes of knee pain tend to be age related. A convenient way to classify knee pain complaints is by age group and by whether the pain is intraarticular, periarticular, or referred (Table 11-3).
| Age | Intraarticular |
|---|---|
| Juvenile (2-10 yrs) |
Adapted from Klippel JH, Dieppe PA: Rheumatology, vol 1-2, ed 2, London, 1998, Mosby.
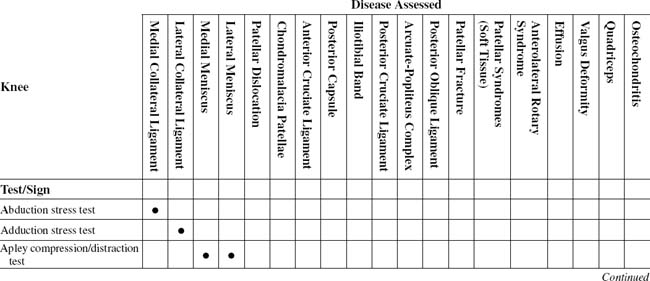
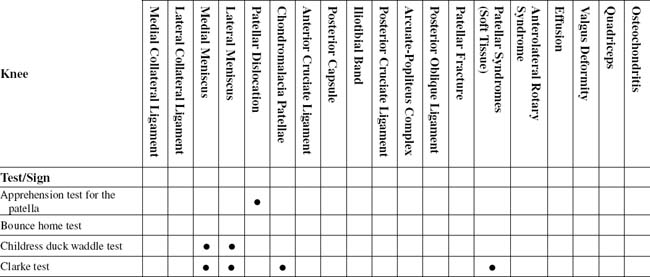
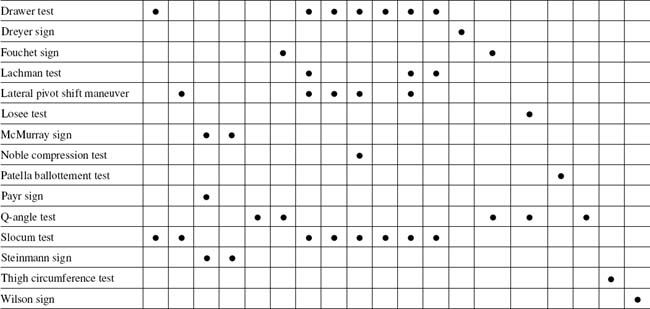
TABLE 11-2 KNEE CROSS-REFERENCE TABLE BY SUSPECTED SYNDROME OR TISSUE
| Anterior cruciate ligament | |
| Arcuate-popliteus complex | |
| Anterolateral rotary syndromes | |
| Chondromalacia patella | |
| Effusion | Patella ballottement test |
| Iliotibial band | |
| Lateral collateral ligament | |
| Lateral meniscus | |
| Medial collateral ligament | |
| Medial meniscus | |
| Osteochondritis | Wilson sign |
| Patellar dislocation | |
| Patellar fracture | Dreyer sign |
| Patellar syndromes | |
| Posterior capsule | |
| Posterior cruciate ligament | |
| Posterior oblique ligament | |
| Quadriceps | Thigh circumference test |
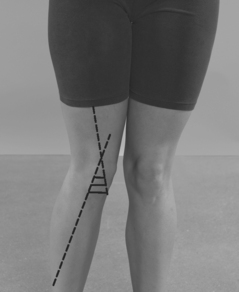
| Valgus deformity | Q-angle test |
ESSENTIAL MOTION ASSESSMENT
The flexion-extension movement of the knee is not a simple hinge motion (Figs. 11-1 and 11-2). As the knee passes through its degrees of flexion and extensions, the imaginary mediolateral axis through which the movement occurs shifts up and down on the femur.


ESSENTIAL MUSCLE FUNCTION ASSESSMENT
The examiner tests the muscles responsible for knee flexion and extension, the hamstrings and quadriceps, respectively (Figs. 11-3 and 11-4).


ABDUCTION STRESS TEST
PROCEDURE

ADDUCTION STRESS TEST
PROCEDURE

APLEY COMPRESSION TEST
PROCEDURE


APPREHENSION TEST FOR THE PATELLA
PROCEDURE


PROCEDURE


CLARKE SIGN
Assessment for Chondromalacia Patellae
ORTHOPEDIC GAMUT 11-12 THREE GROUPS OF PATELLAR MALACIA
PROCEDURE

DRAWER TEST
Assessment for Injury to Some Degree of (1) the Anterior Cruciate Ligament, Especially the Anteromedial Bundle, (2) the Posterolateral Capsule, (3) the Posteromedial Capsule, (4) the Medial Collateral Ligament, Especially the Deep Fibers, (5) the Iliotibial Band, (6) the Posterior Oblique Ligament, (7) the Arcuate-Popliteus Complex, and (8) the Posterior Cruciate Ligament (in Testing Posterior Drawer Movements)
ORTHOPEDIC GAMUT 11-14 GRADES OF KNEE LIGAMENT SPRAINS
ORTHOPEDIC GAMUT 11-16 POSITIVE ANTERIOR DRAWER TEST
In a positive anterior drawer test, the following structures may have been injured to some degree:
PROCEDURE


DREYER SIGN
PROCEDURE

FOUCHET SIGN
PROCEDURE

PROCEDURE

PROCEDURE

PROCEDURE

PROCEDURE

NOBLE COMPRESSION TEST
PROCEDURE



PROCEDURE
SLOCUM TEST
Assessment for Anterolateral Rotary Instability, with Injury to Some Degree of (1) the Anterior Cruciate Ligament, (2) the Posterolateral Capsule, (3) the Arcuate-Popliteus Complex, (4) the Lateral Collateral Ligament, (5) the Posterior Cruciate Ligament, and (6) the Iliotibial Band (Tensor Fascia Lata)
PROCEDURE

PROCEDURE

PROCEDURE

WILSON SIGN
Assessment for Osteochondritis Dissecans of the Knee
ORTHOPEDIC GAMUT 11-25 COMMON ORIGINS OF A LOOSE BODY IN THE KNEE