22
Keratosis pilaris

Keratosis pilaris is characterized by pink, erythematous follicular papules, which are also somewhat scaly.

Discrete erythematous and scaling follicular papules on the lateral upper arms. This is a benign process with a cosmetic impact that is often distressing.

Tiny follicular papules on the lateral cheek. Atopy often accompanies this condition.
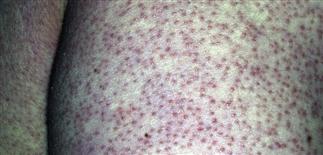
Florid keratosis pilaris on the buttocks of a young child. The erythematous papules involve numerous follicles and are inflammatory.
DESCRIPTION
Keratosis pilaris consists of rough, monomorphic, tiny, follicle-based scaling papules most commonly on the posterolateral aspects of the upper arms but occasionally more widespread, including the anterior and lateral thighs and the buttocks. It results from mild follicular plugging and perifollicular inflammation.
HISTORY
• Keratosis pilaris is very common in young children, peaking in adolescence. • Probably more common in atopic individuals. • Usually asymptomatic but may be somewhat pruritic. • The unusual adult diffuse pattern persists indefinitely. • Keratosis pilaris is common on the face of children and is frequently confused with acne. • Treatment is often desired because of the visible typical location of keratosis pilaris on the extensor upper arms and thighs, and the troubling cosmetic appearance. Otherwise, the condition is generally asymptomatic.
PHYSICAL FINDINGS
• Small, pinpoint follicular papules, and occasionally pustules, remain in the same areas for years. • A red halo appears at the periphery of the keratotic papule. • The skin feels rough, like sandpaper. • Lesions most commonly appear on posterolateral upper arms, anterior and lateral thighs. Occasionally, the condition is generalized and appears on trunk, extensor arms and legs. • No laboratory tests necessary.
TREATMENT
• Many patients seek treatment for cosmesis, because most often the lesions are asymptomatic. • Keratosis pilaris often improves or resolves by adulthood. • Scratching, wearing tight-fitting clothing, or undergoing treatment with abrasive washes or gritty scrubs may aggravate the condition. • Tretinoin (Retin-A) may induce temporary improvement, but irritation is usually unacceptable. • Lac-Hydrin cream 12% or lotion 12% twice a day can reduce roughness and improve appearance. • Low-potency topical steroids may be used in limited courses to temporarily reduce the redness but should not be used on a long-term basis. • The recognition of keratosis pilaris helps avoid inappropriate treatment.






