118
Keloids and hypertrophic scars
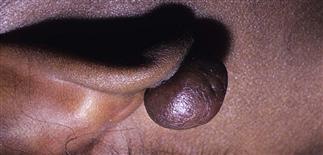
Nodular pedunculated keloid on the posterior earlobe, common with ear piercing.

A keloid is a firm red to purple nodule with telangiectasia that extends beyond the area of trauma.

A keloid formed after an injury. The lesions were injected with triamcinolone 10 mg/cc at intervals of weeks. Early lesions respond better to treatment than older lesions do.

Hypertrophic scars and keloids can arise at any skin site. Most occur on the chest, hand, neck and earlobe. Occasionally, keloids arise spontaneously, without any preceding trauma.
DESCRIPTION
Hypertrophic scars are exuberant scars or healing responses to trauma or injury. Keloids are scars that extend beyond the area of trauma or injury. Most common sites include chest, head, neck. Earlobe is another common site. Surgery, burns, piercing, acne are common insults.
PHYSICAL FINDINGS
• Early, normal scars are usually red to purple and firm during initial weeks of healing. • Itching, tenderness are common for normal scars, hypertrophic scars, keloids.
Hypertrophic scars
Larger and more elevated than normal scars and present for a longer period of time. Have a similar color and texture to those of normal scars. Surface is smooth, dome-shaped, shiny with prominent vessels. One portion of a scar may appear normal, another portion hypertrophied. Unlike keloid scars, they remain confined to site of injury. May regress over time without treatment.
Keloids
By definition, keloid scars extend beyond the area of trauma or injury. Firm, red to violaceous, large, tender nodules. Usually hyperpigmented in African-Americans, red to purple in white people. Depending on type of original injury, lesion may be linear or nodular. In rare instances, keloids may arise spontaneously. This usually occurs on chest and shoulders. Keloid scars show no tendency toward regression and tend to enlarge over time.
TREATMENT
• Patients with history of these scars should be discouraged from cosmetic procedures and piercings. Those requiring surgical procedures in areas at increased risk of abnormal scarring should be advised of this possibility, reminded at time of suture removal. • Hereditary tendency determines who develops hypertrophic scars. Parents of a child who has a cutaneous procedure that results in such scarring need reassurance and a management plan. • Early abnormal scarring typically responds better than older, less active scars. Early intervention advised in these cases. • Intralesional corticosteroid injection probably treatment of choice initially for most. • Radiation therapy and more recently pulse-dye laser therapy have been used for hypertrophic scars, keloids. • Compression therapy and silastic sheeting helpful but inconvenient. • Newer topical silicon-containing gels have been marketed for the treatment of hypertrophic scars, although efficacy in all patients questionable. • Surgical removal or correction of hypertrophic scars and keloids requires experience, careful monitoring. Keloid scars tend to recur often, sometimes larger, after surgical removal. • Combination therapy with intralesional steroids and surgical excision is sometimes required. • Consider referral to a dermatologist or plastic surgeon with an interest in scar removal. • Hypertrophic scars and keloids difficult to eradicate, no matter what procedure is used.






