Multifocal hypodense nodules or masses on CECT with delayed enhancement
• Gastrointestinal
50% of patients with cutaneous Kaposi sarcoma (KS) will have GI tract involvement
Upper GI tract (especially stomach and duodenum) most common, but can affect any part of GI tract
Submucosal nodules or polypoid masses (< 3 cm) most common, although larger infiltrative masses possible
Regional enhancing lymphadenopathy common
Lesions may cause intussusception or obstruction
Submucosal nodules on barium studies with ulceration may appear as “target” or bull’s-eye lesions
• Lymphadenopathy
Most commonly involves retroperitoneal lymph nodes
Commonly hypervascular/avidly enhancing
TOP DIFFERENTIAL DIAGNOSES
• Lymphoma
• Hepatic opportunistic infections
• Intestinal opportunistic infections
• Other causes of hypervascular lymphadenopathy
Hypervascular lymph node metastases
Castleman disease
• Other causes of multiple hepatic/splenic nodules
Metastatic disease from other malignancies
Sarcoid
Hepatic microabscesses or fungal infection
PATHOLOGY
• Associated with human herpesvirus type 8 (HHV8) infection and variable cofactors
• 4 clinical subtypes of KS
Classic (sporadic) KS: Affects elderly men of Eastern European or Mediterranean origin with visceral involvement uncommon
– Indolent cutaneous involvement of lower extremities
Endemic (African) KS: Not associated with HIV, and accounts for up to 1/2 of all cancers in parts of Africa
Iatrogenic (organ transplant-related) KS: Typically develops 1-2 years after transplant, with visceral involvement more likely with heart and liver transplants
Epidemic (AIDS-related) KS: ↓ prevalence with antiretroviral therapies
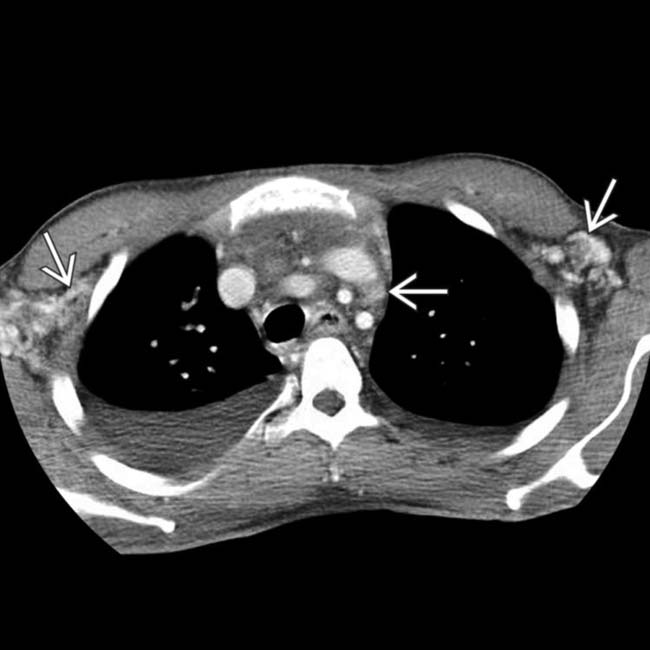
(Left) Axial CECT in a patient with AIDS and disseminated Kaposi sarcoma (KS) shows widespread thoracic lymphadenopathy. Many of the lymph nodes demonstrate hypervascularity , characteristic of KS.
(Right) Axial CECT in the same patient shows widespread abdominal lymphadenopathy with hyperenhancing lymph nodes that help to distinguish KS from lymphoma or other causes of lymphadenopathy.
(Left) Axial CECT through the pelvis in an AIDS patient shows widespread avidly enhancing adenopathy . On excisional biopsy, there was histologic evidence of Castleman disease and KS, both of which can present with avidly enhancing lymph nodes.
(Right) Axial CECT in a patient with HIV and KS shows widespread lymphadenopathy, including nodes in the groin that show hyperenhancement. This patient complained of marked edema of the lower extremities, a common symptom of KS-induced inguinal lymphadenopathy.
TERMINOLOGY
Abbreviations
• Kaposi sarcoma (KS)
Definitions
• Low-grade malignancy arising from mesenchymal lining of blood and lymphatic vessels that primarily affects skin and mucous membranes
IMAGING
General Features
• Best diagnostic clue
Disseminated hypervascular lymphadenopathy with multifocal hepatic or intestinal nodules in patient with known cutaneous KS
Radiographic Findings
• Barium studies of upper or lower gastrointestinal (GI) tract
May show thickened folds or submucosal nodules
Nodules in bowel may ulcerate, appearing as “target” or bull’s-eye lesions
CT Findings
• Liver and spleen: Multifocal nodules or masses (few mm to cm)
Typically hypodense on CECT, but may show delayed enhancement and be invisible on delayed imaging
• GI tract: 50% of patients with cutaneous KS will have GI tract involvement
Upper GI tract (especially stomach and duodenum) most common, but can affect any part of GI tract
Submucosal nodules or polypoid masses (< 3 cm) most common, although larger infiltrative masses possible
– Regional enhancing lymphadenopathy common
May ulcerate, intussuscept, or obstruct
• Lymphadenopathy: Can involve any or all abdominal and pelvic nodal groups
Most commonly involves retroperitoneal lymph nodes
Commonly hypervascular/avidly enhancing
Ultrasonographic Findings
• Hepatomegaly with multiple hyperechoic nodules (< 1 cm)
DIFFERENTIAL DIAGNOSIS
Lymphoma
• Can be indistinguishable from KS, although hyperenhancement of nodes or visceral lesions favors KS
Hepatic Opportunistic Infections
• Fungal infection or microabscesses can mimic KS hepatic nodules
Intestinal Opportunistic Infections
• May cause thickened folds in stomach and bowel
• Discrete large masses or hyperenhancing nodes uncommon with infection
Other Causes of Hypervascular Lymphadenopathy
• Hypervascular lymph node metastases
• Castleman disease
Other Causes of Multiple Nodules in Liver
• Metastatic disease from other malignancies
• Sarcoidosis
• Hepatic microabscesses or fungal infection
PATHOLOGY
General Features
• Etiology
Associated with human herpesvirus type 8 (HHV8) infection and variable cofactors
4 clinical subtypes of KS
– Classic (sporadic) KS
Elderly men of Eastern European or Mediterranean origin
Usually indolent cutaneous involvement of lower extremities
Visceral involvement rare (∼ 10%)
– Endemic (African) KS
Not associated with HIV as risk factor
Accounts for up to 50% of all cancers in certain parts of Africa
Localized, indolent, cutaneous disease in > 50%
Lymphadenopathy ± visceral involvement can be aggressive
– Iatrogenic (organ transplant-related) KS
Affects about 5% of transplant recipients
Mucocutaneous disease in 90%; 40% develop visceral, disseminated disease
Typically develops 1-2 years after organ transplantation
Patients with KS after liver and heart transplants more likely to develop visceral disease (∼ 50%) than kidney transplants (∼ 25%)
– Epidemic (AIDS-related) KS
Prevalence among patients with AIDS is decreasing with use of effective antiretroviral therapies
Most prevalent among homosexual men
In patients with cutaneous KS, autopsy often identifies visceral involvement in lymph nodes (> 70%), lung (50%), GI (50%), and liver/spleen (30%)
Gross Pathologic & Surgical Features
• Purple-brown spongiform nodules in skin, submucosa, nodes, and viscera
CLINICAL ISSUES
Presentation
• Most common signs/symptoms
Purple-brown mucocutaneous spongiform lesions
Similar lesions in viscera on endoscopy or gross inspection
• Other signs/symptoms
Visceral KS rarely causes significant organ dysfunction
– Patients usually succumb to opportunistic infection or lymphoma
Natural History & Prognosis
• Classic form has good prognosis with resection of tumor
• AIDS-related cases usually die from opportunistic infections
Treatment
• Radiation and chemotherapy plus antiretroviral therapy (epidemic type) for symptomatic or disfiguring lesions
Axial CECT in a 36-year-old man with AIDS and cutaneous Kaposi sarcoma shows hyperenhancing lymph nodes in the thorax , typical of nodal involvement by KS.
Axial CECT in the same patient shows abdominal nodal involvement by KS along with liver metastases .
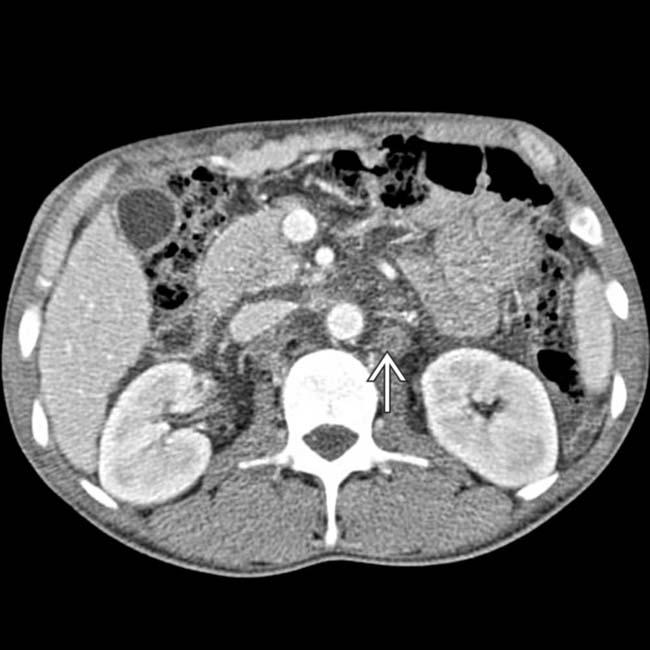
Axial CECT in the same patient shows additional lymphadenopathy from KS.
Axial CECT in a 35-year-old man with AIDS and disseminated KS shows widespread lymphadenopathy, including nodes with hyperdense enhancement .
Axial CECT demonstrates enhancing lymph node masses in both groins encasing the groin vessels. This was found to represent KS on excisional biopsy.













 Classic (sporadic) KS: Affects elderly men of Eastern European or Mediterranean origin with visceral involvement uncommon
Classic (sporadic) KS: Affects elderly men of Eastern European or Mediterranean origin with visceral involvement uncommon
 Endemic (African) KS: Not associated with HIV, and accounts for up to 1/2 of all cancers in parts of Africa
Endemic (African) KS: Not associated with HIV, and accounts for up to 1/2 of all cancers in parts of Africa


 , characteristic of KS.
, characteristic of KS.
 with hyperenhancing lymph nodes that help to distinguish KS from lymphoma or other causes of lymphadenopathy.
with hyperenhancing lymph nodes that help to distinguish KS from lymphoma or other causes of lymphadenopathy.
 . On excisional biopsy, there was histologic evidence of Castleman disease and KS, both of which can present with avidly enhancing lymph nodes.
. On excisional biopsy, there was histologic evidence of Castleman disease and KS, both of which can present with avidly enhancing lymph nodes.
 that show hyperenhancement. This patient complained of marked edema of the lower extremities, a common symptom of KS-induced inguinal lymphadenopathy.
that show hyperenhancement. This patient complained of marked edema of the lower extremities, a common symptom of KS-induced inguinal lymphadenopathy.




























 , typical of nodal involvement by KS.
, typical of nodal involvement by KS.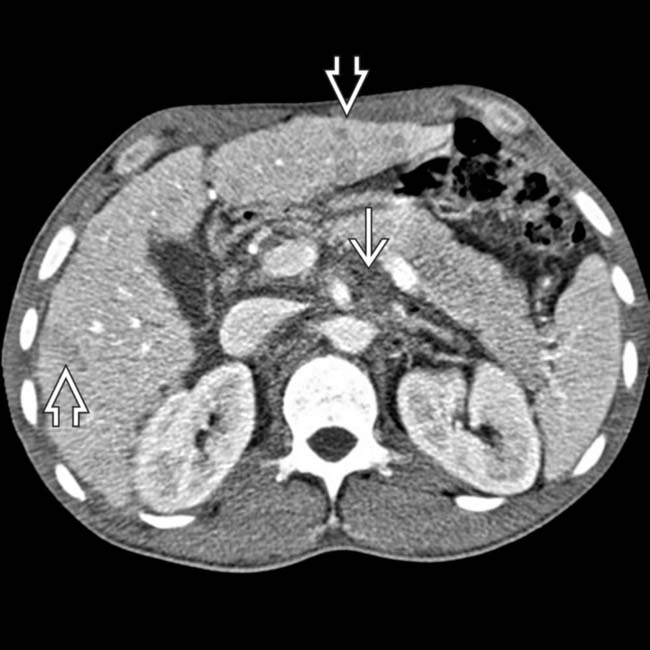
 along with liver metastases
along with liver metastases  .
.
 from KS.
from KS.
 .
.
 in both groins encasing the groin vessels. This was found to represent KS on excisional biopsy.
in both groins encasing the groin vessels. This was found to represent KS on excisional biopsy.

