Jaundice
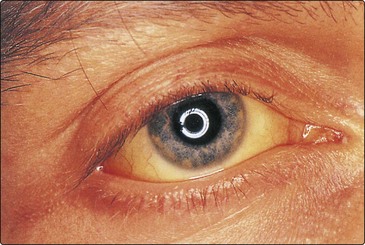
Jaundice is a yellow discoloration of the skin or sclera (Fig 29.1). This is due to the presence of bilirubin in the plasma and is not usually detectable until the concentration is greater than about 50 µmol/L. Normally the bilirubin concentration in plasma is less than 21 µmol/L.
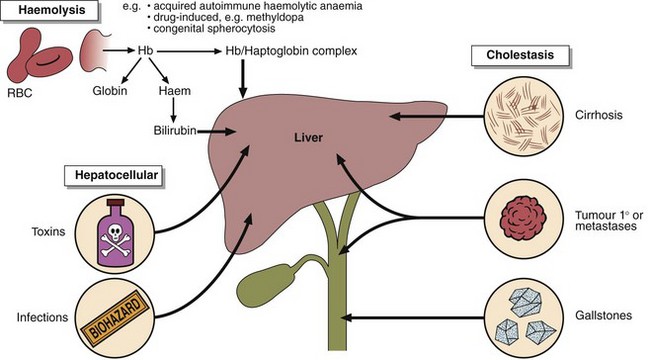
Bilirubin is derived from the tetrapyrrole prosthetic group found in haemoglobin and the cytochromes. It is normally conjugated with glucuronic acid to make it more soluble, and excreted in the bile (Fig 29.2). There are three main reasons why bilirubin levels in the blood may rise (Fig 29.3).
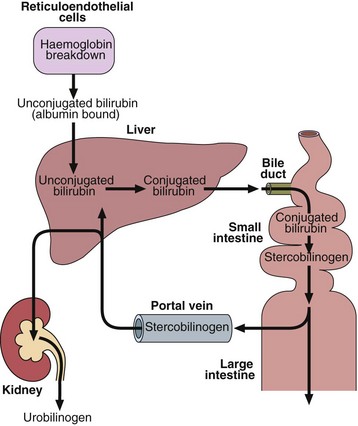
 Haemolysis. The increased haemoglobin breakdown produces bilirubin, which overloads the conjugating mechanism.
Haemolysis. The increased haemoglobin breakdown produces bilirubin, which overloads the conjugating mechanism.


Differential diagnosis
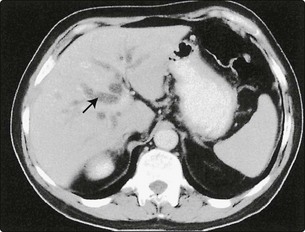
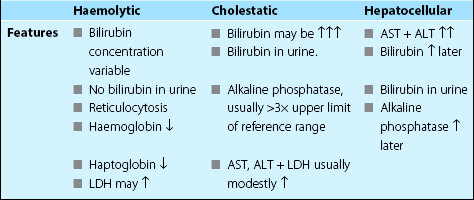
Jaundice may be a consequence of haemolysis, cholestasis or hepatocellular damage. The causes and features of these are summarized in Figure 29.3 and Table 29.1. In addition there are inherited disorders of bilirubin metabolism. Gilbert’s disease is the most common and causes a mild unconjugated hyperbilirubinaemia because of defective hepatic uptake of bilirubin. In this condition bilirubin levels rise on fasting.
Extrahepatic biliary obstruction
Case history 23

 Clinical note
Clinical note