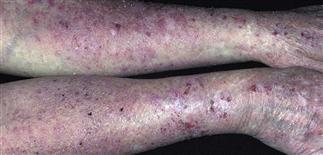
Irritant contact dermatitis

The lips are xerotic and fissured; skin surrounding the lips is erythematous, scaling and chapped appearing. Repeated lip licking is the most common cause of this irritant dermatitis.
Erythema, xerosis, and scaling are common with irritant dermatitis. If no improvement using bland emollients and medium-strength corticosteroid, consider patch testing.

Irritant and allergic dermatitis often appear similar: these hands show erythema, xerosis, scaling, crusting. Look for irritants (repeated washing, soap, solvent, detergent exposure) and allergens.

Dryness, fine scaling, and a faint erythema are typical of a low-grade irritant dermatitis. Daily bland emollient use is helpful.
DESCRIPTION
An eczematous dermatitis often caused by repeated exposure to mild irritants such as water, soaps, solvents, heat, friction. Chronic exposure to mild irritants is common and can result in eczematous changes. Strong irritants include acids, alkalis, wet cement; these chemicals can result in acute lesions of chemical burns. Mild irritants cause dryness, fissuring, erythema; strong irritants produce an immediate reaction of burning, erythema, edema, and possibly vesiculation or ulceration.
HISTORY
• Atopic individuals predisposed and often have more difficult to manage, prolonged course. • Most common type of occupational skin disease. • Critical history: employment, household duties, childcare, hobbies. Jobs characterized by repeated wet work, such as food service, healthcare, childcare, and hairstyling, predispose. • Chronic friction, heat exposure are other causes. • Common irritants: repeated water exposure, detergents, acids, alkaline chemicals, oils, organic solvents, oxidants, reducing agents, coarse fibers. • Potential airborne irritants: fiberglass, formaldehyde, epoxy resins, industrial solvents, glutaraldehyde, sawdust. • May occur with continuous exposure to mild irritants. Once irritation threshold reached, persistent dermatitis results from less exposure. • Low environmental humidity reduces irritation threshold. • Continuous exposure to moisture and wet–dry cycles in areas such as hands, diaper area, or skin around a colostomy may eventually cause eczematous inflammation. • May become complicated by allergy over time.
PHYSICAL FINDINGS
• Most common site: hands. Other sites: eyelids, lips. • Erythema, dryness, painful cracking or fissuring, scaling. • Common: tenderness, burning. • Acute irritant dermatitis may show papules and/or vesicles on erythematous patchy background, with weeping and edema. • Persistent dermatitis results in lichenification, erythematous patches, fissures, excoriations, scaling. • Hyperkeratotic form: scaling, cracking, low-grade erythema may result from repeated mechanical trauma, such as paper handling. • Differential diagnosis: allergic contact dermatitis, atopic dermatitis, psoriasis, tinea.
TREATMENT
• Early diagnosis, treatment, and preventive measures important to avoid chronicity. • Avoidance of or decreased exposure to irritants is critical for skin barrier recovery. • Frequently apply a bland emollient such as Vaseline or Aquaphor to affected skin. • Decrease number of wet–dry cycles resulting from activities, such as repeated hand washing. • Cotton gloves under vinyl gloves may offer good protection (gloves can be ordered online at http://www.allerderm.com). • Encourage appropriate gloves for specific solvent or chemical exposure. • When occupation deemed relevant, consult Material Safety Data Sheet or seek expertise regarding best exposure and protection information. • Use mildest cleanser possible (Cetaphil, Dove, Aquanil). • For irritant hand dermatitis, apply medium- or high-potency topical steroid ointment twice a day for several weeks.






