Iron
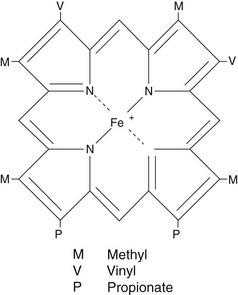
Iron is an essential element in humans, being the central ion in haem, the non-protein component of haemoglobin, myoglobin and the cytochromes (Fig 57.1). Iron deficiency causes a failure in haem synthesis and since haemoglobin is required for delivery of oxygen to the tissues, this leads to anaemia and tissue hypoxia. However, free iron is highly toxic to cells and must be bound to protein at all times.
Iron physiology
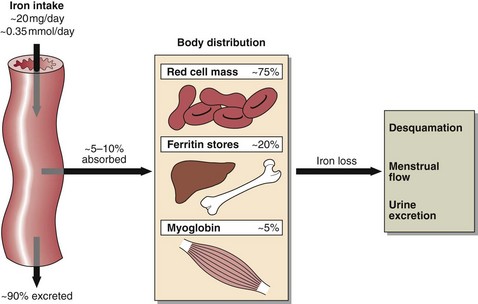
Iron levels are controlled by regulating iron uptake, since there is no mechanism for controlling its excretion. Dietary intake of iron is about 0.35 mmol (20 mg) per day and there are 50–70 mmol (3–4 g) of iron in the body, distributed as shown in Figure 57.2. Iron in the tissue stores is bound to the iron storage proteins ferritin (soluble) and haemosiderin (insoluble). The 1% of body iron in the plasma is associated with the iron binding glycoprotein, transferrin, each molecule of which binds two Fe2+ ions.
Laboratory investigation of iron disorders




Iron deficiency
Iron deficiency anaemia develops in three stages:
1. Depletion of iron stores: confirmed by serum ferritin levels of less than 12 µg/L.
2. Deficient erythropoiesis with normal haemoglobin but increased zinc protoporphyrin. Iron concentration falls, the synthesis of transferrin is increased and the percentage saturation is decreased.
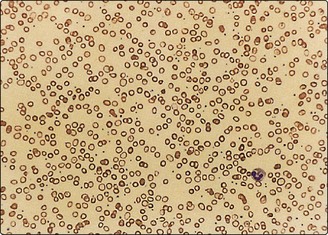
3. Iron deficiency anaemia, in which both iron and haemoglobin are low and there is a microcytic, hypochromic anaemia (Fig 57.3). Low stainable iron is seen in the bone marrow.
Iron overload
 Clinical note
Clinical noteIron poisoning
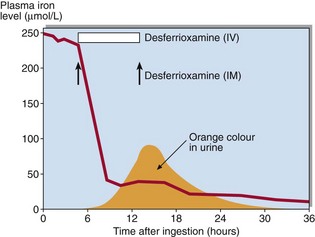
Iron poisoning in children is common and may be life-threatening. Symptoms include nausea and vomiting, abdominal pain and haematemesis. In severe cases, hypotension and coma can result. Serum iron is increased and transferrin is >70% saturated. Treatment is by chelation of the iron in the stomach and the plasma with desferrioxamine. Chelated iron is excreted in the urine as a deep orange coloured complex (Fig 57.4).
Iron
 Iron deficiency is commonly caused by the combination of blood loss and low dietary intake.
Iron deficiency is commonly caused by the combination of blood loss and low dietary intake.
 Iron deficiency can be diagnosed by finding a hypochromic microcytic anaemia.
Iron deficiency can be diagnosed by finding a hypochromic microcytic anaemia.
 Serum ferritin is the most reliable single biochemical test of iron deficiency.
Serum ferritin is the most reliable single biochemical test of iron deficiency.
 Iron overload may arise following repeated blood transfusions.
Iron overload may arise following repeated blood transfusions.

 Accidental iron poisoning in children is an important medical emergency.
Accidental iron poisoning in children is an important medical emergency.
