[level-membership-for-radiology-category] Outer layer = intussuscipiens; inner layer = intussusceptum








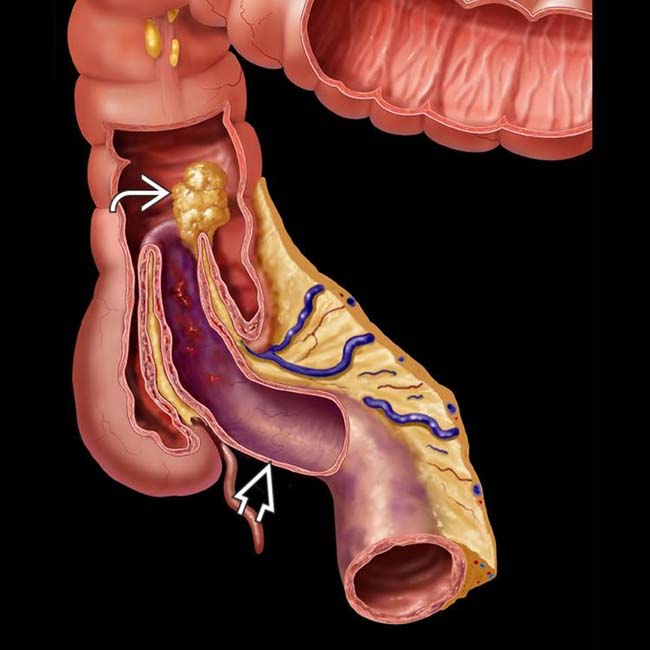
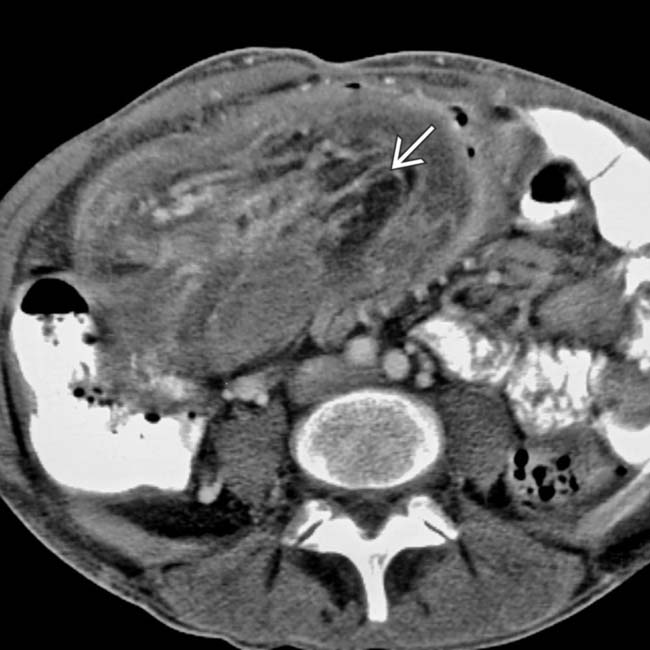
 as the lead mass. Note the vascular compromise and ischemia of the intussusceptum
as the lead mass. Note the vascular compromise and ischemia of the intussusceptum  .
.
 and vessels
and vessels  from an ileocolonic intussusception. The lead mass proved to be carcinoma.
from an ileocolonic intussusception. The lead mass proved to be carcinoma.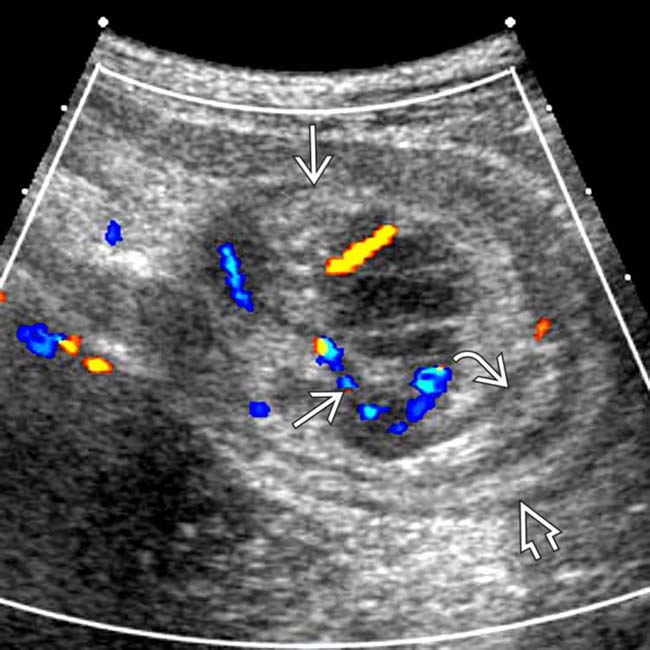
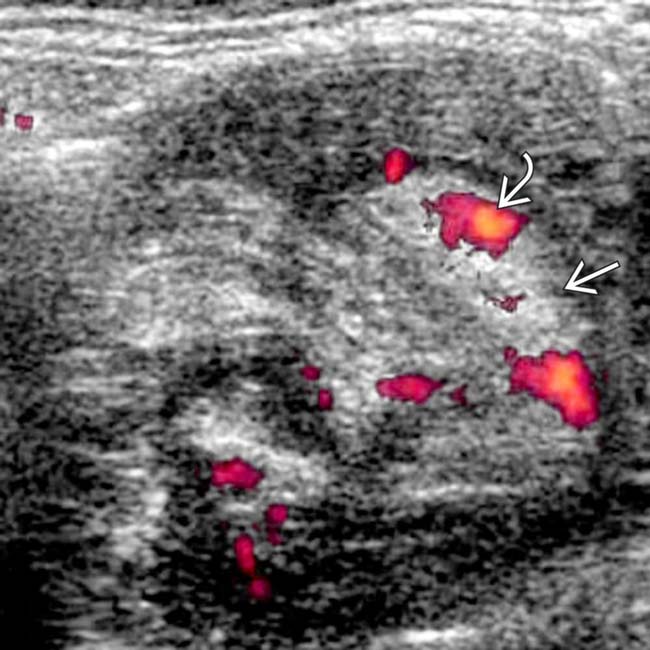
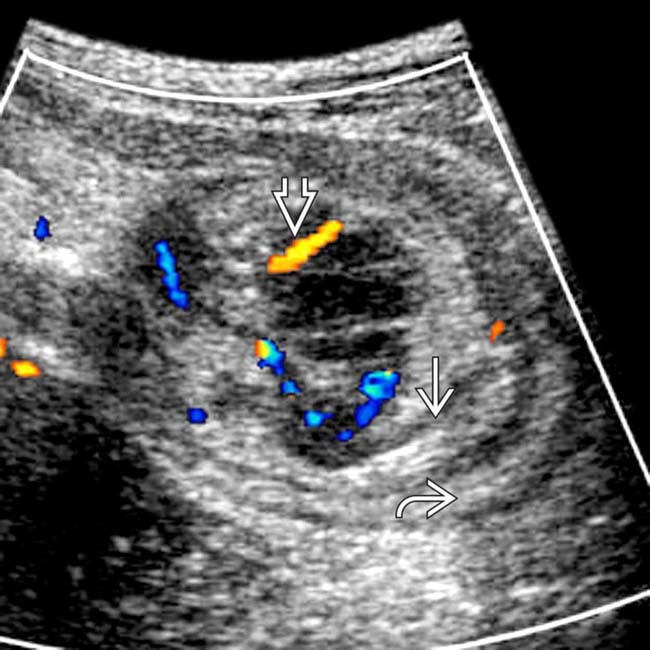
 and 2 echogenic submucosal rings representing intussusceptum
and 2 echogenic submucosal rings representing intussusceptum  and intussuscipiens
and intussuscipiens  .
.
 within the mass, which proved to be a metastatic melanoma.
within the mass, which proved to be a metastatic melanoma.






















































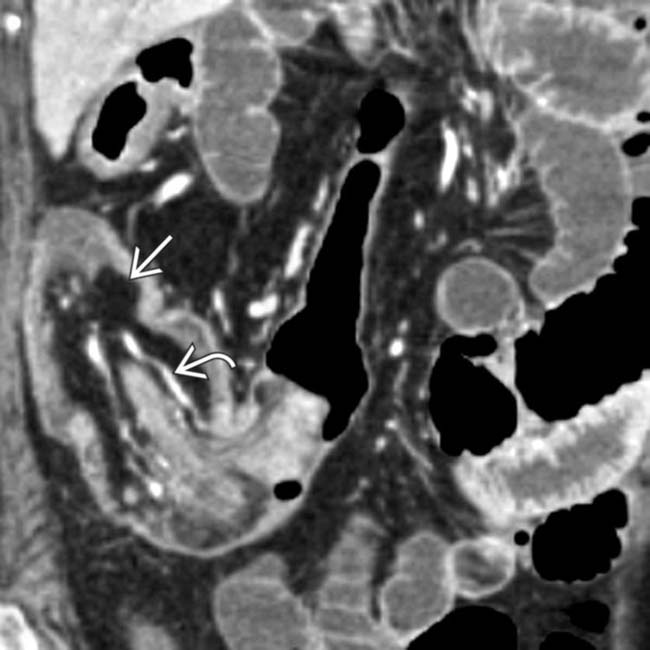
 of the colon wall, while the intussusceptum is a small intestinal segment
of the colon wall, while the intussusceptum is a small intestinal segment  . Mesenteric fat and vessels
. Mesenteric fat and vessels  accompany the intussuscepted small bowel (SB) segment.
accompany the intussuscepted small bowel (SB) segment.
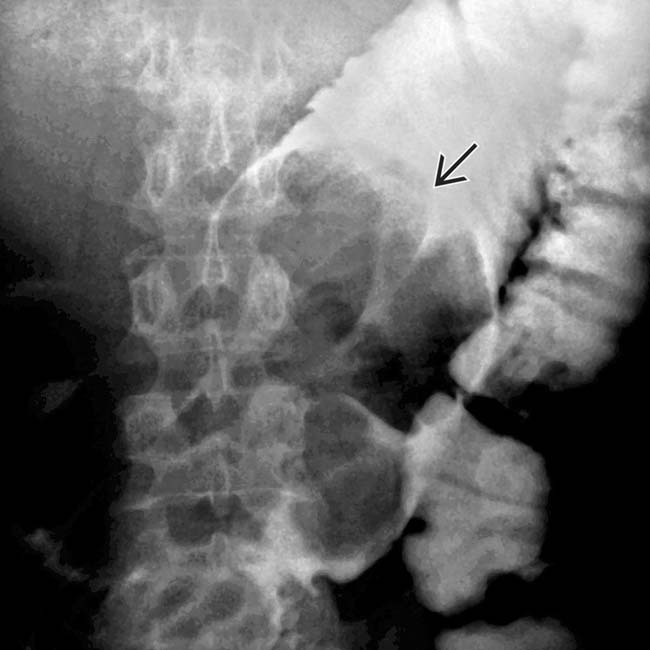
 due to jejunal intussusception. Note the intussuscepted mesenteric fat and vessels
due to jejunal intussusception. Note the intussuscepted mesenteric fat and vessels  .
.
 with its mesenteric fat
with its mesenteric fat  within the contrast opacified lumen of the ascending colon, the intussuscipiens in this case.
within the contrast opacified lumen of the ascending colon, the intussuscipiens in this case.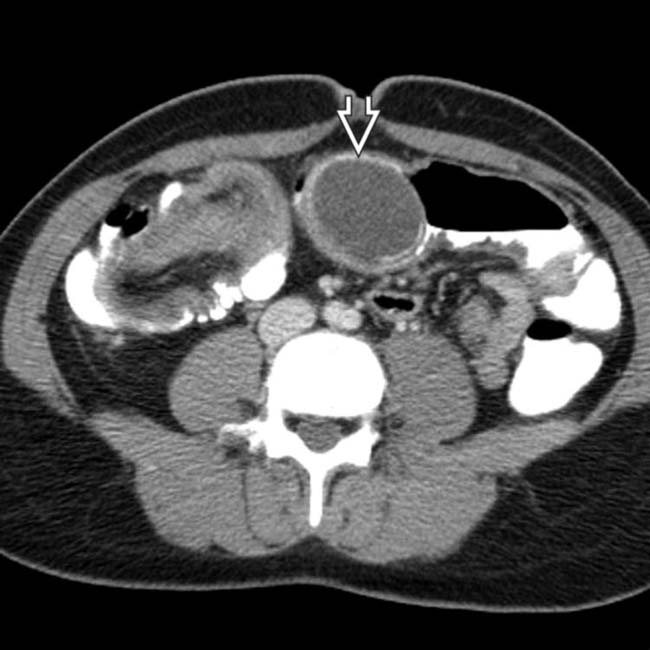
 with a calcified rim, a characteristic appearance of an appendiceal mucocele. Long-segment, obstructing intussusceptions such as this often have a lead mass when seen in adults.
with a calcified rim, a characteristic appearance of an appendiceal mucocele. Long-segment, obstructing intussusceptions such as this often have a lead mass when seen in adults.
 and the mucocele
and the mucocele  as the lead mass.
as the lead mass.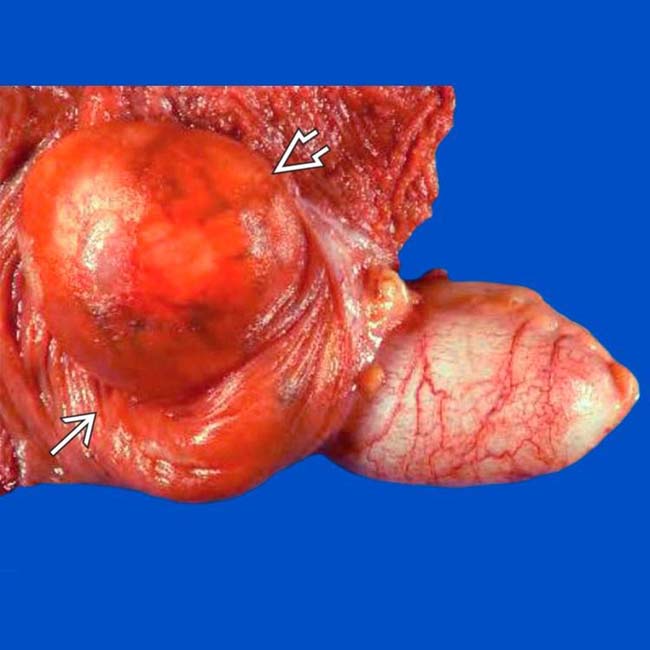
 and the intussusception
and the intussusception  .
.
 with accompanying mesenteric fat and vessels
with accompanying mesenteric fat and vessels  .
.
 .
.
 .
.
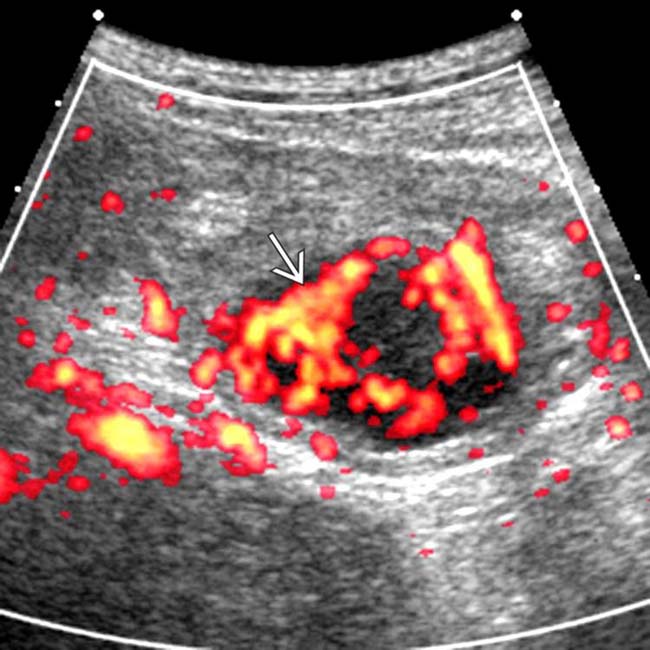
 and intussuscipiens
and intussuscipiens  . Note the invaginated mesenteric vessels
. Note the invaginated mesenteric vessels  .
.
 .
.
 . At surgery, the lead mass was due to inspissated mucoid material within the terminal ileum.
. At surgery, the lead mass was due to inspissated mucoid material within the terminal ileum.

 of the intussusception.
of the intussusception.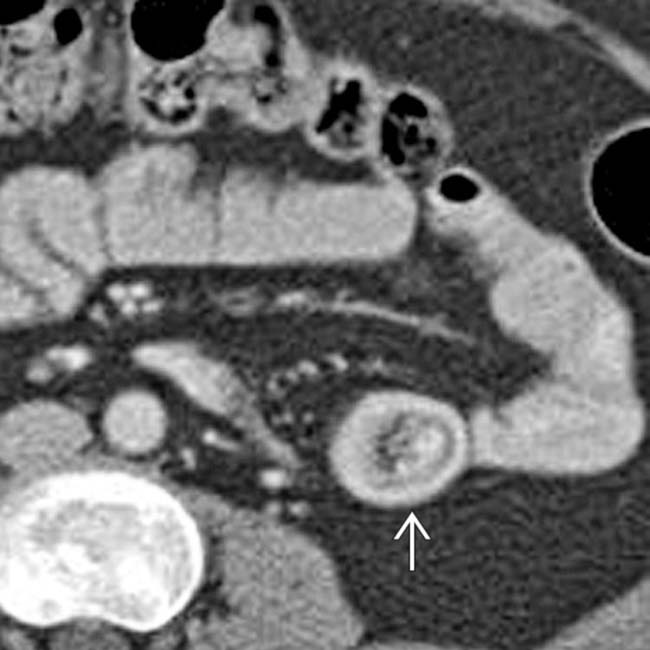
 .
.
 with an accompanying crescent of mesenteric fat. The bowel lumen is dilated due to sprue, not obstruction.
with an accompanying crescent of mesenteric fat. The bowel lumen is dilated due to sprue, not obstruction.
[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Outer layer = intussuscipiens; inner layer = intussusceptum
as the lead mass. Note the vascular compromise and ischemia of the intussusceptum . and vessels from an ileocolonic intussusception. The lead mass proved to be carcinoma. and 2 echogenic submucosal rings representing intussusceptum and intussuscipiens . within the mass, which proved to be a metastatic melanoma.IMAGING
General Features
Imaging Recommendations
• Best imaging tool
Buy Membership for Radiology Category to continue reading. Learn more here
[/not-level-membership-for-radiology-category]
