Intravenous fluid therapy
 Does this patient need IV fluids?
Does this patient need IV fluids?

 How much fluid should be given?
How much fluid should be given?


Which IV fluids should be given?
The list of intravenous fluids that is available for prescription in many hospital formularies is long and potentially bewildering. However, with a few exceptions, many of these fluids are variations on the three basic types of fluid shown in Figure 13.1.
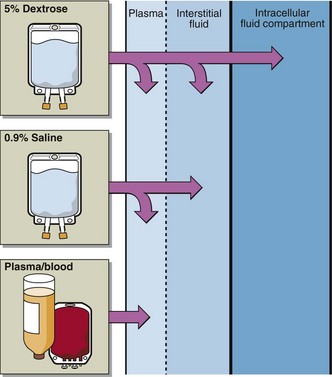
Fig 13.1 The three types of fluid usually used in intravenous fluid therapy are shown here with the different contributions they make to the body fluid compartments.
 Plasma, whole blood, or plasma expanders. These replace deficits in the vascular compartment only. They are indicated where there is a reduction in the blood volume due to blood loss from whatever cause. Such solutions are sometimes referred to as ‘colloids’ to distinguish them from ‘crystalloids’. Colloidal particles in solution cannot pass through the (semipermeable) capillary membrane, in contrast with crystalloid particles like sodium and chloride ions, which can. This is why they are confined to the vascular compartment, whereas sodium chloride (‘saline’) solutions are distributed throughout the entire ECF.
Plasma, whole blood, or plasma expanders. These replace deficits in the vascular compartment only. They are indicated where there is a reduction in the blood volume due to blood loss from whatever cause. Such solutions are sometimes referred to as ‘colloids’ to distinguish them from ‘crystalloids’. Colloidal particles in solution cannot pass through the (semipermeable) capillary membrane, in contrast with crystalloid particles like sodium and chloride ions, which can. This is why they are confined to the vascular compartment, whereas sodium chloride (‘saline’) solutions are distributed throughout the entire ECF.


How should the fluid therapy be monitored?
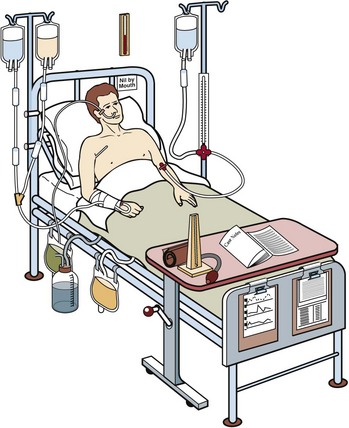
The best place to study monitoring of IV fluid replacement in practice is in the intensive care setting. Here, comprehensive monitoring of a patient’s fluid and electrolyte balance (Fig 13.2) allows the prescribed fluid regimen to be tailored to the patient’s individual requirement.
 Clinical note
Clinical note
Assessing a patient’s fluid and electrolyte status has as much, if not more, to do with clinical skill than biochemical interpretation. Look at the patient in Figure 13.2 and think about what information is available. Your answer may include consideration of the following:
 case records (details of patient history, examination)
case records (details of patient history, examination)
 examination of patient (JVP, CVP, pulse, BP, presence of oedema, chest sounds, skin turgor)
examination of patient (JVP, CVP, pulse, BP, presence of oedema, chest sounds, skin turgor)
 fluid balance and nursing charts (BP, pulse, temperature, fluid-input and output)
fluid balance and nursing charts (BP, pulse, temperature, fluid-input and output)
 nasogastric and surgical wound drainage, in addition to urinary catheter bag
nasogastric and surgical wound drainage, in addition to urinary catheter bag









