63 Intravascular Injections
Ultrasound guidance for regional blocks appears to reduce but not eliminate the vascular puncture risk. This is similar to what has been reported for ultrasound guidance for other interventions.1
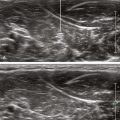
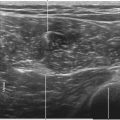
Small-volume test injections (0.5-1 mL) are useful for detecting intravascular injections.2 If the injection is not visualized, it should be stopped immediately. It is best to presume intravascular injection or some other adverse event.
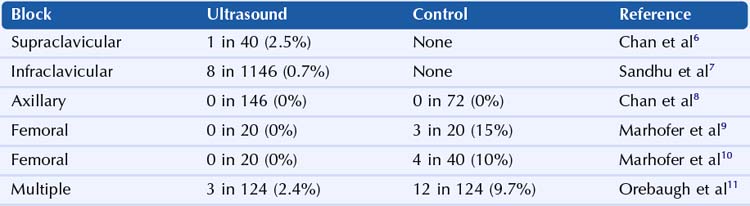
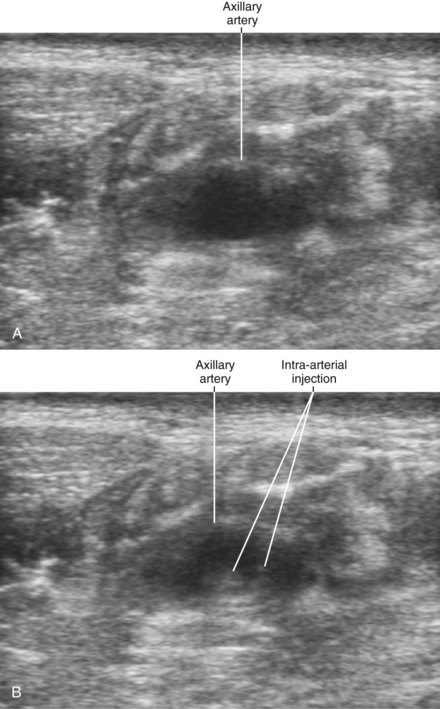
Despite this favorable safety profile, intravascular injection with systemic toxicity has been reported with ultrasound guidance.3,4 Another concern is that probe compression may prevent detection of intravenous injection by collapsing the vein after puncture.5 It is difficult to assess the incidence of these problems from case reports, but these events are likely uncommon and primarily relate to limitations in needle tip visibility. Vascular puncture rates reported from clinical studies of ultrasound-guided regional blocks are listed in Table 63-1.6–11
Table 63-1 Vascular Puncture Rates Reported from Clinical Studies of Ultrasound-Guided Regional Blocks
1 Randolph AG, Cook DJ, Gonzales CA, et al. Ultrasound guidance for placement of central venous catheters: a meta-analysis of the literature. Crit Care Med. 1996;24:2053–2058.
2 VadeBoncouer TR, Weinberg GL, Oswald S, et al. Early detection of intravascular injection during ultrasound-guided supraclavicular brachial plexus block. Reg Anesth Pain Med. 2008;33:278–279.
3 Loubert C, Williams SR, Hélie F, et al. Complication during ultrasound-guided regional block: accidental intravascular injection of local anesthetic. Anesthesiology. 2008;108:759–760.
4 Zetlaoui PJ, Labbe JP, Benhamou D. Ultrasound guidance for axillary plexus block does not prevent intravascular injection. Anesthesiology. 2008;108:761.
5 Robards C, Clendenen S, Greengrass R. Intravascular injection during ultrasound-guided axillary block: negative aspiration can be misleading. Anesth Analg. 2008;107:1754–1755.
6 Chan VW, Perlas A, Rawson R, et al. Ultrasound-guided supraclavicular brachial plexus block. Anesth Analg. 2003;97:1514–1517.
7 Sandhu NS, Manne JS, Medabalmi PK, et al. Sonographically guided infraclavicular brachial plexus block in adults: a retrospective analysis of 1146 cases. J Ultrasound Med. 2006;25:1555–1561.
8 Chan VW, Perlas A, McCartney CJ, et al. Ultrasound guidance improves success rate of axillary brachial plexus block. Can J Anaesth. 2007;54:176–182.
9 Marhofer P, Schrogendorfer K, Wallner T, et al. Ultrasonographic guidance reduces the amount of local anesthetic for 3-in-1 blocks. Reg Anesth Pain Med. 1998;23:584–588.
10 Marhofer P, Schrögendorfer K, Koinig H, et al. Ultrasonographic guidance improves sensory block and onset time of three-in-one blocks. Anesth Analg. 1997;85:854–857.
11 Orebaugh SL, Williams BA, Kentor ML. Ultrasound guidance with nerve stimulation reduces the time necessary for resident peripheral nerve blockade. Reg Anesth Pain Med. 2007;32:448–454.