64 Intraneural Injections
Safety issues for ultrasound in regional anesthesia practice have been raised by several authors.1,2 Tremendous controversy and debate surround this field, particularly in regard to the subject of intraneural injection.
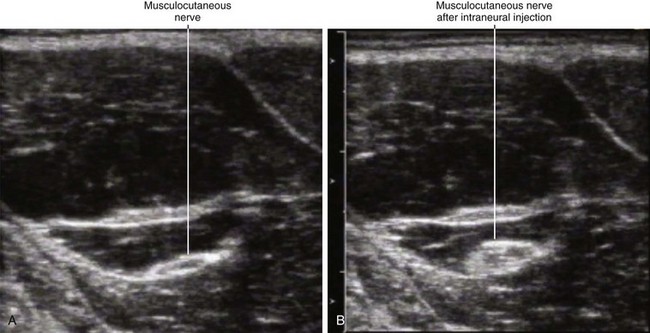
A large number of seemingly innocuous intraneural injections imaged with ultrasound have been reported.1,3,4 In these cases, although nerve expansion from injection was reported, no loss of nerve border integrity was detected. All these intraneural injections were believed to be low pressure. Most of these harmless intraneural injections have been detected by retrospective review of ultrasound recordings of blocks and were not recognized online in real time. All these intraneural injections were in nerves with high collagen content and polyfascicular architecture. There have been no reported cases of intraneural injections in monofascicular nerves, which would more likely result in functional damage.
We have yet to establish the sonographic signs of intraneural injections that produce functional damage. To date, there has been only one published report of sonographic nerve imaging following nerve injury resulting from needle injection.5 Sonography cannot distinguish between subepineurial and subperineurial needle tip placement. Subperineurial injection is thought to be more harmful.6
Intraneural injections have been dichotomized into high-pressure and low-pressure types.7,8 The low-pressure type has not been associated with injury and may be common in clinical practice. Collateral damage may be the mechanism of adjacent fiber injury after high-pressure injection (nerve blast injury from explosion with surrounding nerve fascicles damaged).
Ultrasound may be able to identify some factors that influence the chance of nerve injury during regional anesthetics. Nerve echotexture may play an important role in perioperative nerve injuries. Polyfascicular nerves contain more protective connective tissue than monofascicular nerves. The outcomes after monofascicular nerve injuries are probably worse than after polyfascicular injuries.9
Nerves are usually mobile and distensible structures. However, if nerve fascicles become trapped on both sides of the advancing needle, paresthesia often occurs as the needle crosses into or even through the nerve. The complex architecture of peripheral nerves in regard to somatotopic orientation of motor and sensory fibers may account for the variability in mechanically and electrically evoked responses. Ultrasound also can identify proximity to underlying structures that are an unyielding surface. Nerve blocks performed near bone have been associated with a high incidence of nerve dysfunction.10
Clinical Pearls
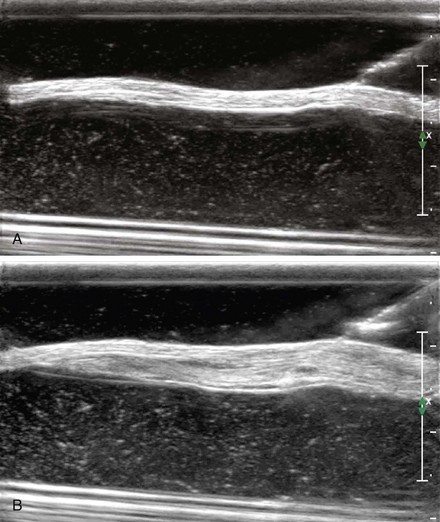
• Traumatic nerve lesions are characterized by nerve enlargement, nerve hyperemia, loss of fascicular discrimination, swelling proximal to the injured segment, and change in nerve caliber.
• Intraneural needle tip placement is often only recognized after injection (and even then, by retrospective review of recorded images rather than online).
• Factors that influence regenerative capacity of peripheral nerves include diabetes, preexisting neuropathy, age, and others.
• Adverse symptoms have been reported after intentional intraneural injection of local anesthetics.11
• Adverse neurologic outcome related to needle injection has been reported without sonographic evidence of intraneural injection.12
1 Schafhalter-Zoppoth I, Zeitz ID, Gray AT. Inadvertent femoral nerve impalement and intraneural injection visualized by ultrasound. Anesth Analg. 2004;99:627–628.
2 Chan VW, Brull R, McCartney CJ, et al. An ultrasonographic and histological study of intraneural injection and electrical stimulation in pigs. Anesth Analg. 2007;104:1281–1284.
3 Bigeleisen PE. Nerve puncture and apparent intraneural injection during ultrasound-guided axillary block does not invariably result in neurologic injury. Anesthesiology. 2006;105:779–783.
4 Russon K, Blanco R. Accidental intraneural injection into the musculocutaneous nerve visualized with ultrasound. Anesth Analg. 2007;105:1504–1505.
5 Graif M, Seton A, Nerubai J, et al. Sciatic nerve: sonographic evaluation and anatomic-pathologic considerations. Radiology. 1991;181:405–408.
6 Gentili F, Hudson A, Kline DG, et al. Peripheral nerve injection injury: an experimental study. Neurosurgery. 1979;4:244–253.
7 Selander D, Sjostrand J. Longitudinal spread of intraneurally injected local anesthetics: an experimental study of the initial neural distribution following intraneural injections. Acta Anaesthesiol Scand. 1978;22:622–634.
8 Hadzic A, Dilberovic F, Shah S, et al. Combination of intraneural injection and high injection pressure leads to fascicular injury and neurologic deficits in dogs. Reg Anesth Pain Med. 2004;29:417–423.
9 Sunderland S. The anatomy and physiology of nerve injury. Muscle Nerve. 1990;13:771–784.
10 Lofstrom B, Wennberg A, Wien L. Late disturbances in nerve function after block with local anaesthetic agents: an electroneurographic study. Acta Anaesthesiol Scand. 1966;10:111–122.
11 Lee J, Lee YS. Percutaneous chemical nerve block with ultrasound-guided intraneural injection. Eur Radiol. 2008;18:1506–1512.
12 Koff MD, Cohen JA, McIntyre JJ, et al. Severe brachial plexopathy after an ultrasound-guided single-injection nerve block for total shoulder arthroplasty in a patient with multiple sclerosis. Anesthesiology. 2008;108:325–328.