May ulcerate with gas ± contrast medium entering cavity
• CT: Discrete mass in wall; no signs of invasion or metastases
Helps distinguish lipoma (fat density) and other mediastinal masses (e.g., mediastinal cyst)
TOP DIFFERENTIAL DIAGNOSES
• Mediastinal tumor
• Normal mediastinal structures
• Esophageal carcinoma
• Foreign body
CLINICAL ISSUES
• Asymptomatic: No treatment
• Large, symptomatic lesions: Enucleation or esophageal resection with gastric interposition
DIAGNOSTIC CHECKLIST
• Most intramural masses are benign (unlike gastric tumors)
• Leiomyomas are much more common than GIST in esophagus (but not in stomach)
• Calcifications suggest leiomyoma; almost never occur in other benign/malignant esophageal tumors
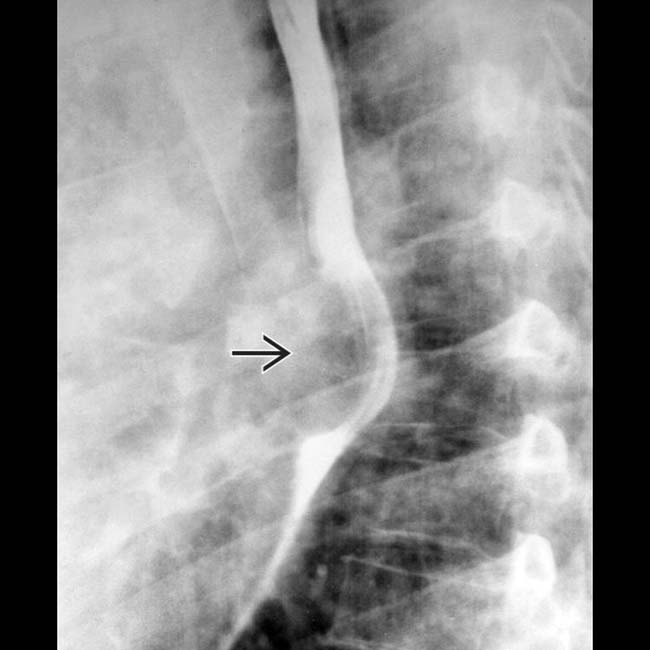
(Left) Film from a barium esophagram demonstrates a mass causing eccentric narrowing of the distal lumen. The mass forms obtuse angles with the wall, and the esophageal folds and mucosa are intact. A leiomyoma was enucleated endoscopically.
(Right) Single-contrast esophagram shows an en face view of an intramural mass in the distal esophagus with central ulceration due to leiomyoma. The traction diverticulum is an incidental finding.
(Left) Coronal CECT in a 24-year-old man shows a huge, soft tissue density mass that envelops and displaces the distal esophagus . Small foci of calcification are noted. The mass was resected and proved to be a benign leiomyoma arising from the esophageal wall.
(Right) Axial CECT in a 73-year-old woman shows a huge esophageal mass with a large central ulceration that contains gas due to communication with the esophageal lumen. The central cavitation is typical of a GIST; the esophagus is an unusual site.
TERMINOLOGY
Definitions
• Benign mass composed of 1 or more tissue elements of esophageal wall
IMAGING
General Features
• Best diagnostic clue
Intramural mass with smooth surface and slightly obtuse borders on barium esophagram
• Size
1 cm to > 10 cm
• Other
Types include leiomyoma, GI stromal tumor, granular cell, lipoma, hemangioma, hamartoma
Radiographic Findings
• Fluoroscopic-guided barium studies
Discrete mass; solitary (most common) or multiple
Round or ovoid filling defects sharply outlined by barium on each side (en face view)
– Overlying mucosa may ulcerate
Smooth surface lesion, with upper and lower borders forming right or slightly obtuse angles with adjacent esophageal wall (profile view)
Narrowed (tangential view) or stretched and widened (en face view) esophageal lumen
– Varying degree of obstruction
Leiomyoma ± amorphous or punctate calcifications
Esophageal gastrointestinal stromal tumor (GIST)
– May be large mass
– May ulcerate with gas ± contrast medium entering cavity
Granular cell: Distal 1/3 > middle 1/3; 0.5-2.0 cm
Hamartoma
– Large and pedunculated; mimics fibrovascular polyp
May ulcerate with gas ± contrast medium entering cavity
• CT: Discrete mass in wall; no signs of invasion or metastases
Helps distinguish lipoma (fat density) and other mediastinal masses (e.g., mediastinal cyst)
TOP DIFFERENTIAL DIAGNOSES
• Mediastinal tumor
• Normal mediastinal structures
• Esophageal carcinoma
• Foreign body
CLINICAL ISSUES
• Asymptomatic: No treatment
• Large, symptomatic lesions: Enucleation or esophageal resection with gastric interposition
DIAGNOSTIC CHECKLIST
• Most intramural masses are benign (unlike gastric tumors)
• Leiomyomas are much more common than GIST in esophagus (but not in stomach)
• Calcifications suggest leiomyoma; almost never occur in other benign/malignant esophageal tumors
(Left) Film from a barium esophagram demonstrates a mass causing eccentric narrowing of the distal lumen. The mass forms obtuse angles with the wall, and the esophageal folds and mucosa are intact. A leiomyoma was enucleated endoscopically.
(Right) Single-contrast esophagram shows an en face view of an intramural mass in the distal esophagus with central ulceration due to leiomyoma. The traction diverticulum is an incidental finding.
(Left) Coronal CECT in a 24-year-old man shows a huge, soft tissue density mass that envelops and displaces the distal esophagus . Small foci of calcification are noted. The mass was resected and proved to be a benign leiomyoma arising from the esophageal wall.
(Right) Axial CECT in a 73-year-old woman shows a huge esophageal mass with a large central ulceration that contains gas due to communication with the esophageal lumen. The central cavitation is typical of a GIST; the esophagus is an unusual site.
TERMINOLOGY
Definitions
• Benign mass composed of 1 or more tissue elements of esophageal wall
IMAGING
General Features
• Best diagnostic clue
Intramural mass with smooth surface and slightly obtuse borders on barium esophagram
• Size
1 cm to > 10 cm
• Other
Types include leiomyoma, GI stromal tumor, granular cell, lipoma, hemangioma, hamartoma
Radiographic Findings
•
Buy Membership for Radiology Category to continue reading. Learn more here


 Smooth surface lesion, with upper and lower borders of lesion forming right or slightly obtuse angles with adjacent esophageal wall (profile view)
Smooth surface lesion, with upper and lower borders of lesion forming right or slightly obtuse angles with adjacent esophageal wall (profile view)



 causing eccentric narrowing of the distal lumen. The mass forms obtuse angles with the wall, and the esophageal folds and mucosa are intact. A leiomyoma was enucleated endoscopically.
causing eccentric narrowing of the distal lumen. The mass forms obtuse angles with the wall, and the esophageal folds and mucosa are intact. A leiomyoma was enucleated endoscopically.
 due to leiomyoma. The traction diverticulum
due to leiomyoma. The traction diverticulum  is an incidental finding.
is an incidental finding.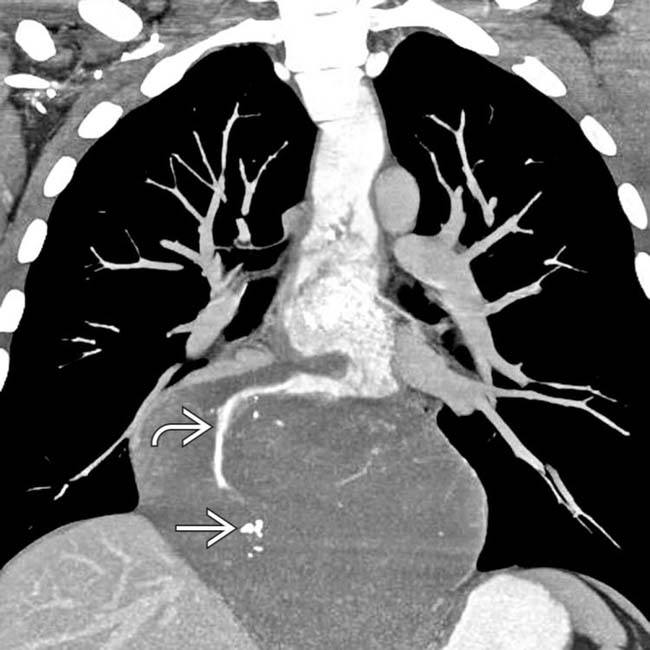
 . Small foci of calcification
. Small foci of calcification  are noted. The mass was resected and proved to be a benign leiomyoma arising from the esophageal wall.
are noted. The mass was resected and proved to be a benign leiomyoma arising from the esophageal wall.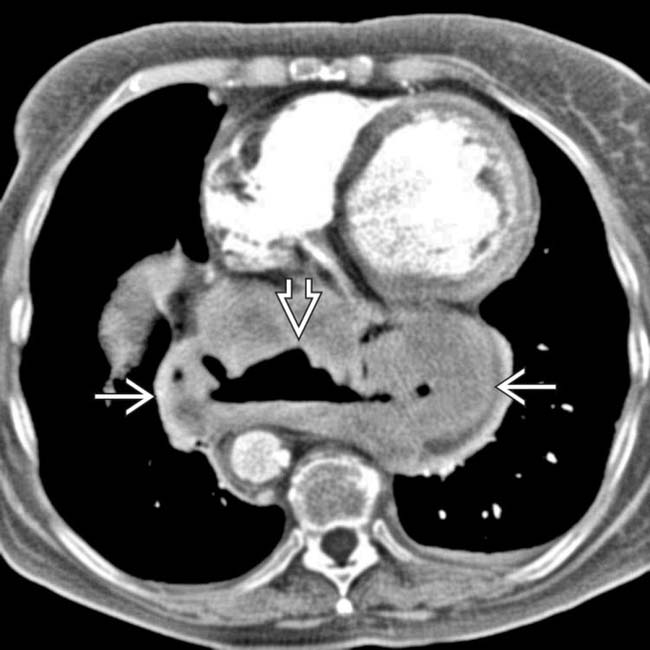
 with a large central ulceration
with a large central ulceration  that contains gas due to communication with the esophageal lumen. The central cavitation is typical of a GIST; the esophagus is an unusual site.
that contains gas due to communication with the esophageal lumen. The central cavitation is typical of a GIST; the esophagus is an unusual site.


 Smooth surface lesion, with upper and lower borders forming right or slightly obtuse angles with adjacent esophageal wall (profile view)
Smooth surface lesion, with upper and lower borders forming right or slightly obtuse angles with adjacent esophageal wall (profile view)























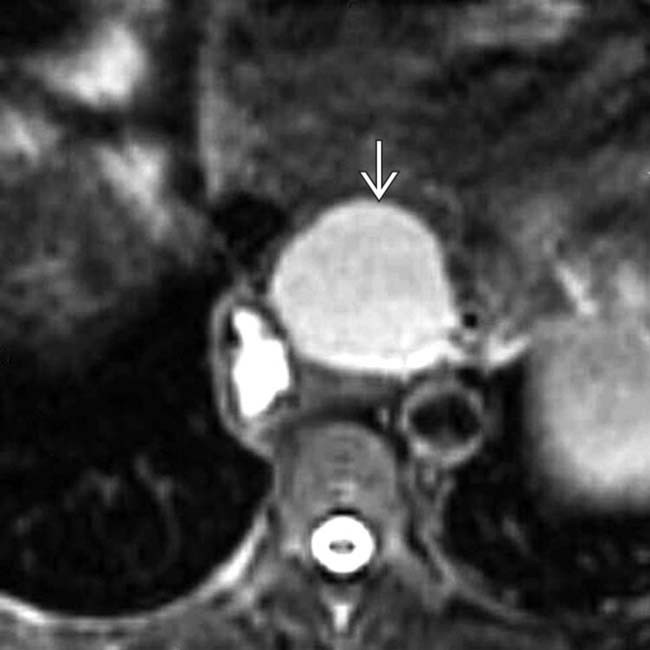
 as complex fluid intensity.
as complex fluid intensity.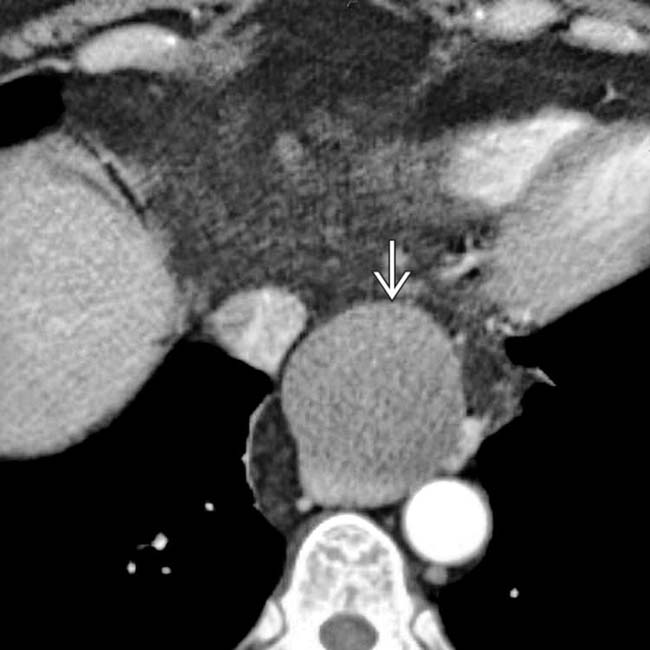
 displacing the distal esophagus (duplication or foregut cyst).
displacing the distal esophagus (duplication or foregut cyst).
 , and right angle or obtuse angle with wall.
, and right angle or obtuse angle with wall.