[level-membership-for-anesthesiology-category]
Intra-cardiac Masses and Devices
Al Solina, F. Luke Aldo and Salvatore Zisa
Cardiac Masses: A mass by any other name, is still a mass. Or is it?
You may remember from high school physics that mass is simply a quantity of matter. Under the right set of circumstances, it can even be converted into a predictable amount of energy. But that’s not what we are talking about here. Cardiac masses come in a variety of shapes, sizes, locations, consistencies, and clinical significance. They can be characterized primarily into real masses, and normal anatomical structures that masquerade as masses. Real cardiac masses can be further characterized as being benign or malignant, and as being primary or metastatic. In order to differentiate between these possibilities it is important to understand normal anatomy, the physics involved with imaging artifacts (see Chapter 5), and the characterization of real cardiac masses. Echocardiography has been utilized to image cardiac masses since the 1950s, and can be used to characterize the anatomy and pathophysiological consequences of the mass. Although a mass may be histologically benign, it may muck up the normal function of the heart by interfering with chamber filling or valve function, and therefore not be benign from a physiological perspective.
Masses that are Not Really Masses
Atrial Anatomic Variants
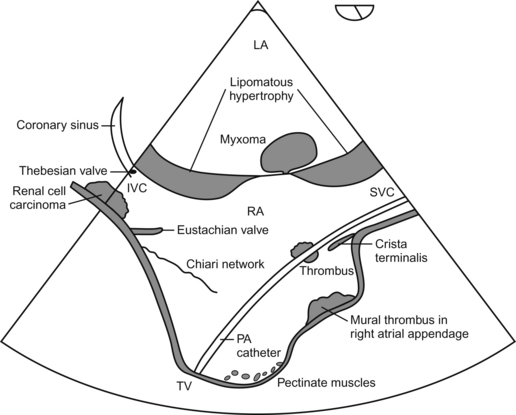
 Chiari network—having little to do with communications or information technology, this network is a filamentous embryological remnant located in the RA.
Chiari network—having little to do with communications or information technology, this network is a filamentous embryological remnant located in the RA.


 Eustachian valve—an embryological remnant, located at the junction between the IVC and the RA, and directed towards the fossa ovalis of the interatrial septum.
Eustachian valve—an embryological remnant, located at the junction between the IVC and the RA, and directed towards the fossa ovalis of the interatrial septum.



Ventricular Anatomic Variants







Masses that Really are Masses
“Benign” primary cardiac masses: these masses are “benign” in their tissue characterization, but may misbehave and cause functional disturbances attributable to their anatomical location!
 Myxoma—most common primary tumor, seen most frequently in the LA. Can be quite large and interfere with valvular function. Have a non-homogeneous appearance. Female preponderance. May commonly be seen attached to a stalk from the LA side of the interatrial septum. May be associated with systemic embolization.
Myxoma—most common primary tumor, seen most frequently in the LA. Can be quite large and interfere with valvular function. Have a non-homogeneous appearance. Female preponderance. May commonly be seen attached to a stalk from the LA side of the interatrial septum. May be associated with systemic embolization.






Malignant Primary Cardiac Masses
 Angiosarcoma—is the most common primary malignancy of the heart, and displays a fondness for the right atria of middle-aged men. They may be either intracavitary or infiltrative. They are associated with a grave prognosis.
Angiosarcoma—is the most common primary malignancy of the heart, and displays a fondness for the right atria of middle-aged men. They may be either intracavitary or infiltrative. They are associated with a grave prognosis.

 Mesothelioma—affecting men more often than women, is typically seen between ages 30 and 50.
Mesothelioma—affecting men more often than women, is typically seen between ages 30 and 50.
Schematic Representation of Common Cardiac “Masses”
Metastatic Cardiac Masses






Imaging Modalities Utilized to Characterize Cardiac Masses
 2-D—it is critically important to evaluate cardiac masses utilizing a multitude of views in order to appreciate the true functional anatomic features of the mass.
2-D—it is critically important to evaluate cardiac masses utilizing a multitude of views in order to appreciate the true functional anatomic features of the mass.
 3-D—real time 3-D imaging has been demonstrated to better elucidate the anatomical relationships of intracardiac masses, and may alter surgery when utilized intraoperatively.
3-D—real time 3-D imaging has been demonstrated to better elucidate the anatomical relationships of intracardiac masses, and may alter surgery when utilized intraoperatively.

Questions
1. Which is the most common primary malignant cardiac tumor in children?
2. The most common primary tumor affecting valves is:
3. A filamentous embryological remnant located in the RA
4. Which of the following is/are true regarding angiosarcoma?
A It is the most common primary malignancy of the heart
B It displays a fondness for the right atria of middle-aged men
C They may be either intracavitary or infiltrative
5. Which of the following statements is/are true?
A Myxomas demonstrate relative avascularity
B Carcinoid primarily affects the left side of the heart
C Lung cancer is the most common type to metastasize to the heart
6. Which of the following is/are true?
A The Eustachian valve is associated with the coronary sinus
B Most vegetations occur on the right side of the heart
C The Thebesian valve is associated with the junction between the RA and IVC
7. Which is are true regarding papillary fibroelastoma?
A The most common primary tumor affecting valves
B It resembles a small (<1 cm) vegetation, but is usually seen on the downstream side of a valve
C Found more frequently in association with left heart valves in patients greater than 50 years of age
8. Which is/are true of fibromas?
A Second most common benign cardiac tumor in children (rhabdomyoma is first)
B Most frequently seen in the ventricle
C Although benign in tissue type, may be associated with impaired ventricular filling and/or arrythmias
Answers
[/level-membership-for-anesthesiology-category][not-level-membership-for-anesthesiology-category]
Intra-cardiac Masses and Devices
Al Solina, F. Luke Aldo and Salvatore Zisa
Cardiac Masses: A mass by any other name, is still a mass. Or is it?
You may remember from high school physics that mass is simply a quantity of matter. Under the right set of circumstances, it can even be converted into a predictable amount of energy. But that’s not what we are talking about here. Cardiac masses come in a variety of shapes, sizes, locations, consistencies, and clinical significance. They can be characterized primarily into real masses, and normal anatomical structures that masquerade as masses. Real cardiac masses can be further characterized as being benign or malignant, and as being primary or metastatic. In order to differentiate between these possibilities it is important to understand normal anatomy, the physics involved with imaging artifacts (see Chapter 5), and the characterization of real cardiac masses. Echocardiography has been utilized to image cardiac masses since the 1950s, and can be used to characterize the anatomy and pathophysiological consequences of the mass. Although a mass may be histologically benign, it may muck up the normal function of the heart by interfering with chamber filling or valve function, and therefore not be benign from a physiological perspective.
Masses that are Not Really Masses
Atrial Anatomic Variants
Chiari network—having little to do with communications or information technology, this network is a filamentous embryological remnant located in the RA.
Eustachian valve—an embryological remnant, located at the junction between the IVC and the RA, and directed towards the fossa ovalis of the interatrial septum.
Ventricular Anatomic Variants
Masses that Really are Masses
“Benign” primary cardiac masses: these masses are “benign” in their tissue characterization, but may misbehave and cause functional disturbances attributable to their anatomical location!
Myxoma—most common primary tumor, seen most frequently in the LA. Can be quite large and interfere with valvular function. Have a non-homogeneous appearance. Female preponderance. May commonly be seen attached to a stalk from the LA side of the interatrial septum. May be associated with systemic embolization.
[/not-level-membership-for-anesthesiology-category]
