81 Internuclear ophthalmoplegia
Salient features
Examination
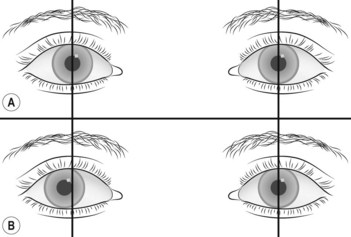
• Nystagmus is more prominent in the abducting eye (Harris’ sign)
• Abduction in either eye is normal, whereas adduction is impaired (Fig. 81.1): there is dissociation of eye movements. On covering the abducting eye, the adduction in the other eye is normal.
Advanced-level questions
What are the mechanisms to elicit conjugate gaze?
There are four mechanisms for eliciting conjugate gaze in any direction.
• The saccadic system involves voluntary gaze (even when the eyes are shut). Pathways mediating saccadic gaze arise in the frontal lobe and pass to the pontine gaze centre.
• The pursuit system allows the subject to follow a moving object. Pathways mediating pursuit movements arise in the parieto-occipital lobe and pass to the pontine gaze centre.
• The optokinetic system involves the restoration of gaze despite movements from the outside world (e.g. while a subject is sitting in a railway train and looking out of the window, the eyes move slowly as the train moves, to be followed by rapid corrective movement back to the initial position of gaze). This is tested with a hand-held drum bearing vertical black and white stripes. Optokinetic nystagmus is often disturbed even before damage to the pursuit system is apparent.
• The vestibulo-ocular system involves correction of gaze for movements of the head. This is achieved by inputs from the labyrinths and neck proprioreceptors to the brainstem. The patient is asked to fixate to the examiner’s face and the head is briskly rotated by the examiner from side to side or up and down (doll’s head manoeuvre). In supranuclear gaze palsy, these vestibulo-ocular reflex eye movements are preserved, despite the absence of both saccadic and pursuit movements. Caloric tests are used to demonstrate the vestibulo-ocular reflex.
Notes
1 Diplopia is not a feature of defects in conjugate gaze.
2 The centres for saccadic and pursuit movements in the cerebral hemispheres control deviation of the eyes towards the opposite side of the body. These pathways descend towards the brainstem and cross before they reach the pons.
3 The centres for conjugate vertical gaze lie in the midbrain.
4 The centres for conjugate downward vertical gaze are not well localized and lesions both in the midbrain and at the level of the foramen magnum can cause defects of voluntary downgaze.






