[level-membership-for-surgery-category]
Chapter 7 Intensive care
Acute Respiratory Distress Syndrome (ARDS)
Causes
| Direct injury | Indirect injury |
|---|---|
| Pulmonary contusion | Septicaemia |
| Gastric aspiration | Major trauma |
| Fat and amniotic fluid embolus | Cardiopulmonary bypass |
| Infection | Massive blood transfusion |
| Cytotoxic drugs | Prolonged hypotension |
| Smoke inhalation | Hepatic and renal failure |
| Oxygen toxicity | Disseminated intravascular coagulation |
Pathophysiology
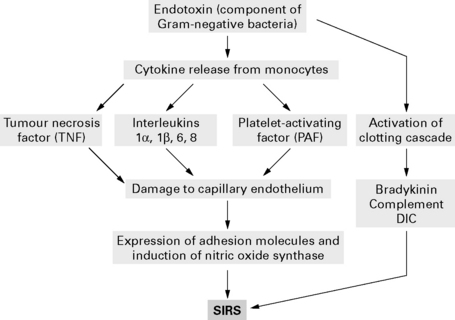
Activated neutrophils adhere to endothelial cells and release inflammatory mediators, including oxygen-free radicals and proteases, to cause lung damage. Direct lung damage or endotoxins alone are sufficient to damage endothelial cells with cytokine release and an inflammatory cascade (Fig. 7.1).
Treatment
Treat underlying cause
Other methods of improving oxygenation
 and arterial oxygenation. Long-term benefits have not been proven.
and arterial oxygenation. Long-term benefits have not been proven.Secondary infection. High risk of secondary infection reduced with prophylactic antibiotics.
Acutely Ill Patients in Hospital: Recognition of and Response to Acute Illness in Adults in Hospital
National Institute for Clinical Excellence 2007
Guidance
Chan K.P., Stewart T.E., Mehta S. High-frequency oscillatory ventilation for adult patients with ARDS. Chest. 2007;131:1907-1916.
Dernaika T.A., Keddissi J.I., Kinasewitz G.T. Update on ARDS: beyond the low tidal volume. Am J Med Sci. 2009;337:360-367.
Malarkkan N., Snook N.J., Lumb A.B. New aspects of ventilation in acute lung injury. Anaesthesia. 2003;58:647-667.
McLuckie A. High-frequency oscillation in acute respiratory distress syndrome (ARDS). Br J Anaesth. 2004;93:322-323.
Moloney E.D., Griffiths M.J.D. Protective ventilation of patients with acute respiratory distress syndrome. Br J Anaesth. 2004;92:261-270.
NICE. Quick reference guide. Acutely ill patients in hospital. NICE clinical guideline, 2007;50. www.nice.org.uk/nicemedia/pdf/CG50QuickRefGuide.pdf.
Rouby J.-J., Consstantin .J-M., Girardi C.R., et al. Mechanical ventilation in patients with acute respiratory distress syndrome. Anesthesiology. 2004;101:228-234.
Cardiovascular System
Inotropes
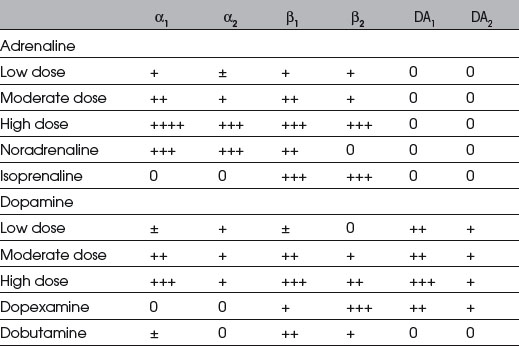
If shock persists despite adequate volume replacement and vital organ perfusion is jeopardized, inotropic drugs may be required to improve blood pressure and cardiac output (Table 7.2).
Adrenergic receptor function
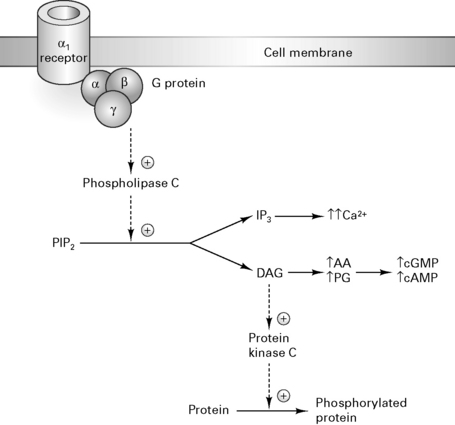
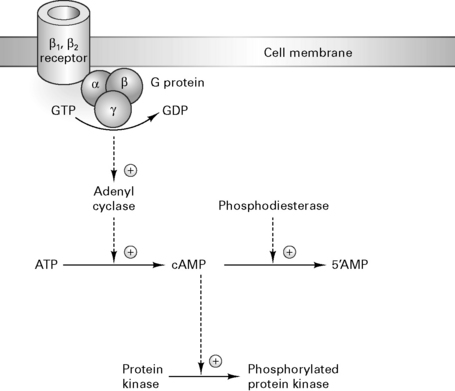
α1 receptors activate phospholipase C which cleaves phosphoinositol 4,5-biphosphate (PIP2) to diacylglycerol (DAG) and inositol triphosphate (IP3). DAG activates protein kinase C to release arachidonic acid which increases cGMP synthesis (Fig. 7.2). Activation of β1, β2 and dopamine (D1) receptors triggers the conversion of ATP to cAMP, activating protein kinase C and triggering protein phosphorylation which causes tachycardia and increases contractility (Fig. 7.3).
Pulmonary artery catheters
Indications
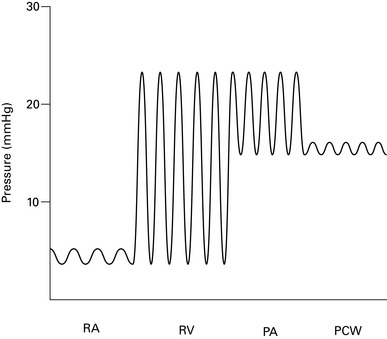
Complications
Table 7.3 Complications of pulmonary artery catheter insertion
| Associated with insertion | Associated with catheter presence |
|---|---|
| Pneumothorax/haemothorax | Infection of catheter or site |
| Haematoma | Pulmonary thrombosis/infarct |
| Cardiac arrhythmias | Cardiac arrhythmias |
| Arterial puncture | Valve damage/endocarditis |
| Pulmonary artery perforation | Pulmonary artery erosion |
| Catheter knotting | Thrombocytopenia |
| Cardiac valve damage |
Cardiac output monitoring
Invasive techniques



Non-invasive techniques
American Society of Anesthesiologists Task Force on Pulmonary Artery Catheterization. Practice guidelines for pulmonary artery catheterization. Anesthesiology. 2003;99:988-1014.
Antonelli M., Levy M., Andrews P.J., et al. Hemodynamic monitoring in shock and implications for management. International Consensus Conference. Intensive Care Med. 2007;33:575-590.
Dawson S., Jhanji S., Pears J.R.M. Cardiac output monitoring: basic science and clinical application. Anaesthesia. 2008;63:172-181.
Jhanji S., Dawson J., Pearse R.M. Cardiac output monitoring: basic science and clinical application. Anaesthesia. 2008;63:172-181.
Klein A.A., Snell A., Nashef S.A., et al. The impact of intra-operative transoesophageal echocardiography on cardiac surgical practice. Anaesthesia. 2009;64:947-952.
Moppett I., Shajar M. Transoesophageal echocardiography. BJA CEPD Rev. 2001;1:72-75.
Van Lieshout J.J., Wesseling K.H. Continuous cardiac output by pulse contour analysis? Br J Anaesth. 2001;86:467-469.
Fluid and Electrolyte Balance
The neonate has a greater proportion of body water and in a different distribution than the adult (Fig. 7.5). More fluid is distributed within the extracellular compartment (interstitial and plasma volume) compared with the adult, resulting in a larger volume of distribution for water-soluble drugs. A large proportion of interstitial fluid is excreted within the first few weeks after birth and adult levels are attained by adolescence.
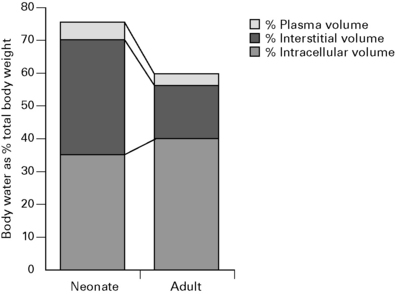
A 70 kg male has about 42 kg of water distributed through three body compartments.



Normal fluid requirements
Postoperative fluid requirements
Intravenous fluids administered perioperatively during minor gynaecological surgery reduce morbidity, particularly nausea and dizziness. However, blood coagulation appears to be accelerated by haemodilution with saline, and in patients undergoing elective abdominal surgery, the incidence of DVT was four times greater than in the fluid-restricted group (Janvrin et al 1980).
Albumin
Benefits of correcting hypoalbuminaemia are unclear. A prospective randomized study of 475 ICU patients comparing albumin and gelatin solutions failed to show any benefit (Stockwell et al 1992). In 70 children with burns, albumin supplementation failed to improve morbidity or mortality (Greenhalgh et al 1995). In septic patients, albumin infusions will only increase COP for a relatively short period. Increased capillary permeability results in >60% of albumin leaving the intravascular compartment within 4 h, potentially worsening oedema.
A controversial systematic review by the Cochrane Group of 23 randomized controlled trials found that the risk of death was 6% greater in the group treated with albumin compared with those receiving crystalloids or no treatment (Cochrane Injuries Group 1998). The Committee on Safety of Medicines now advises doctors to restrict the use of, and take special care when using, human albumin, but states that there is ‘insufficient evidence of harm to warrant withdrawal of albumin’. Hypoalbuminaemia in itself is not an appropriate indication. Risks of hypervolaemia and cardiovascular overload warrant monitoring in patients receiving albumin.
Intravenous fluids
Crystalloids
0.9% normal saline (per 1000 mL)
Colloid versus crystalloid controversy (Table 7.4)
| Advantages | Disadvantages | |
|---|---|---|
| Crystalloid | Cheap | Larger volumes needed |
| Replaces extravascular loss | Small ↑ in plasma volume | |
| Increased GFR | Peripheral and pulmonary oedema | |
| Minimal effect on clot quality | ||
| Colloid | Smaller volumes needed | Risk of anaphylaxis |
| Prolonged ↑ in plasma volume | Relatively expensive | |
| Reduced peripheral oedema | Coagulopathy | |
| Poor clot quality |
British Consensus Guidelines on Intravenous Fluid Therapy for Adult Surgical Patients
Summary and recommendations
Preoperative fluid management
Intraoperative fluid management
Postoperative fluid and nutritional management
Fluid management in acute kidney injury (AKI)
Boldt J. The balanced concept of fluid resuscitation. Br J Anaesth. 2007;99:312-315.
Chappell D., Hofmann-Kiefer K., Conzen P., et al. A rational approach to perioperative fluid management. Anesthesiology. 2008;109:723-740.
Choi P.T.L., Yip G., Quinonez L.G., et al. Crystalloids vs colloids in fluid resuscitation: a systematic review. Crit Care Med. 1999;27:200-210.
Cochrane Injuries Group. Human albumin administration in critically injured patients: systematic review of randomised controlled trials. BMJ. 1998;317:235-240.
Greenhalgh D.G., Housinger T.A., Kagan R.J., et al. Maintenance of serum albumin levels in pediatric burn patients: a prospective, randomized trial. J Trauma. 1995;39:67-74.
Grocott M.P.W., Mythen M., Gan T.J. Perioperative fluid management and clinical outcome in adults. Anesth Analg. 2005;100:1093-1106.
Janvrin S.B., Davies G., Greenhalgh R.M. Postoperative deep vein thrombosis caused by intravenous fluids during surgery. Br J Surg. 1980;67:690-693.
Powell-Tuck J., Gosling P., Lobo D.N., et al. British Consensus Guidelines on Intravenous Fluid Therapy for Adult Surgical Patients, 2008 www.ics.ac.uk/intensive_care_professional/standards_and_guidelines/british_consensus_guidelines_on_intravenous_fluid_therapy_for_adult_surgical_patients__giftasup__2008.
Rassam S.S., Counsell D.J. Perioperative fluid therapy. Contin Edu Anaesth, Crit Care Pain. 2005;5:161-165.
Stockwell M.A., Soni N., Riley B. Colloid solutions in the critically ill. A randomised comparison of albumin and polygeline. 1. Outcome and duration of stay in the intensive care unit. Anaesthesia. 1992;47:3-6.
Strandvik G.F. Hypertonic saline in critical care: a review of the literature and guidelines for use in hypotensive states and raised intracranial pressure. Anaesthesia. 2009;64:990-1003.
Methicillin Resistant Staphylococcus Aureus (MRSA)
Risk factors for infection are:
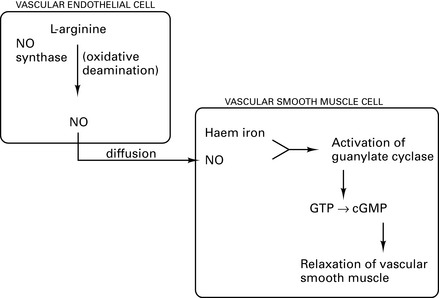
Nitric Oxide
In 1987, nitric oxide (NO) was identified as an endothelium-derived relaxing factor. It is a free radical acting as a local transcellular messenger through binding to transition metals within enzymes such as guanylate cyclase. About 1 mM of endogenous nitric oxide is synthesized per day. The synthesis and actions of NO are shown in Figure 7.6. NO is involved in:
Non-Invasive Ventilation
Nutrition
Malnutrition
Assessment of malnutrition
Effects of malnutrition
Respiratory. Decreased inspiratory force and FVC; weaning more difficult.
GI. Decreased gut motility, gut atrophy and increased gut permeability to intestinal bacteria.
Starvation and stress result in different rates of malnutrition and changes in catabolic pathways (Table 7.5).
Table 7.5 Effect of starvation and stress on energy expenditure and malnutrition
| Starvation | Stress | |
|---|---|---|
| Energy expenditure | + | +++ |
| R:Q | 0.7 | 0.8–0.85 |
| Malnutrition | + | +++ |
| Rate of malnutrition | + | +++ |
Nutritional support
Composition
Monitor electrolytes daily, monitor blood sugar every 48 h, monitor liver function tests weekly.
Daily requirements (per 24 h)
The following are also required:
Bistrian B.R., McCowen K.C. Nutritional and metabolic support in the adult intensive care unit: key controversies. Crit Care Med. 2006;34:1525-1531.
Napolitano L., Cresci G., Martindale R.G., et al. Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient: Society of Critical Care Medicine and American Society for Parenteral and Enteral Nutrition: Executive Summary. Crit Care Med. 2009;37:1757-1761.
Oxygen Transport
Physiology
Oxygen cascade (PO2) (kPa)
| Oxygen content (mL/dL) | ||
|---|---|---|
| Arterial | Mixed venous | |
| Total | 20.0 | 15.0 |
| Attached to Hb | 19.7 | 14.9 |
| Dissolved | 0.3 | 0.1 |
| 2.0 (100% O2) | ||
| Saturation | 97% | 73% |
Oxygen content

CaO2 = arterial oxygen content
(1.3 × Hb × SaO2) – i.e. 1 g Hb, when completely saturated, binds 1.3 mL O2
(0.003 × PaO2) = amount of O2 dissolved in plasma = 0.003 mL.mmHg−1.

 = cardiac output.
= cardiac output.
 × (CaO2 − CVO2) (Fick equation)
× (CaO2 − CVO2) (Fick equation)
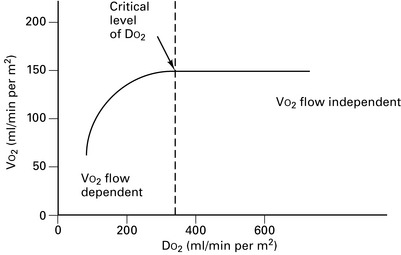
Oxygen extraction ratio
The oxygen extraction ratio (O2ER) is the fractional uptake of oxygen from the capillary bed.

Renal Replacement Therapy
Renal replacement therapy therefore aims to remove excess water and remove unwanted solutes.
Immediate management of oliguria/acute renal failure
Principles
Water removal
Solute removal
This can be achieved by either diffusion or ultrafiltration.
Diffusion across a semi-permeable membrane. This is movement of solutes across a semi-permeable membrane from an area of high concentration to one of low concentration. A concentration gradient is therefore always necessary for diffusion to occur. Molecules of a smaller MW will move across the membrane more readily than those with a larger MW (Fig. 7.8). A semi-permeable membrane has a defined pore size; any molecule exceeding this will not be able to pass through.
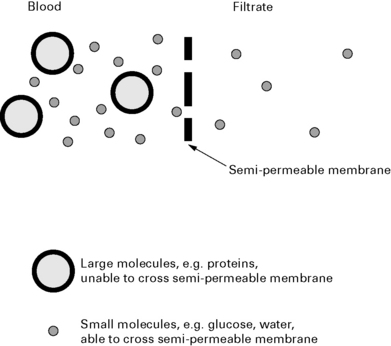
This is the principle utilized for dialysis.
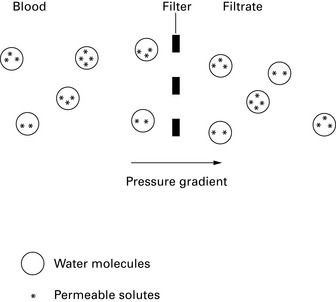
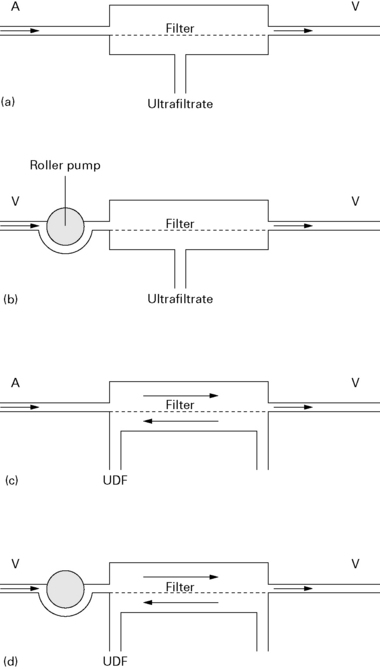
Ultrafiltration (convective transport) is the bulk movement of water molecules containing permeable solutes through a semi-permeable membrane (Fig. 7.9). Water molecules are small and can pass through all semi-permeable membranes. The driving force for ultrafiltration can be either an osmotic gradient or hydrostatic pressure. Haemofiltration is based on the principle of ultrafiltration.
Types of filtration circuit
Replacement fluids
Bicarbonate ions are lost by filtration, resulting in a metabolic acidosis unless replaced.
Bicarbonate ions are not present in most replacement solutions because:
Hall N.A., Fox A.J. Renal replacement therapies in critical care. Contin Edu Anaesth, Crit Care Pain. 2006;6:197-202.
Joannidis M. Continuous renal replacement therapy in sepsis and multisystem organ failure. Semin Dial. 2009;22:160-164.
Mallick N.P., Gokal R. Haemodialysis. Lancet. 1999;353:737-742.
Short A., Cumming A. ABC of intensive care. Renal support. BMJ. 1999;319:41-44.
Scoring Systems
APACHE (acute physiology and chronic health evaluation)
| Mean blood pressure | Respiratory rate | Temperature |
| Pulse | Glasgow Coma Scale | Urine output |
| Haematocrit | White cell count | Blood pH |
| PaO2 | PaCO2 | Serum sodium |
| Serum albumin | Serum bilirubin | Serum glucose |
| Serum creatinine | Blood urea nitrogen |
Beck D.H., Taylor B.L., Millar B., et al. Prediction of outcome from intensive care: a prospective cohort study comparing Acute Physiology and Chronic Health Evaluation II and III prognostic systems in a United Kingdom intensive care unit. Crit Care Med. 1997;25:9-15.
Bouch D.C., Thompson J.P. Severity scoring systems in the critically ill, Contin Edu Anaesth. Crit Care Pain. 2008;8:181-185.
Le Gall J.R., Lemeshow S., Saulnier F. A new simplified acute physiology score (SAPS II) based on a European/North American multicenter study. JAMA. 1993;270:2957-2963.
Lemeshow S., Teres D., Klar J., et al. Mortality probability models (MPM II) based on an international cohort of intensive care unit patients. JAMA. 1993;270:2478-2486.
Zimmerman J.E., Kramer A.A., McNair D.S., et al. Acute physiology and chronic health evaluation (APACHE) IV: hospital mortality assessment for today’s critically ill patients. Crit Care Med. 2006;34:1297-1310.
Sedation
Sepsis
Surviving Sepsis Campaign – Sepsis Care Bundles
Sepsis resuscitation bundle (to be achieved within 6 h of presentation)
Dellinger R.P., Levy M.M., Carlet J.M., et al. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock, 2008. Crit Care Med. 2008;36:296-327.
Fletcher S.J., Quinn A.C. The surviving sepsis campaign and sepsis care bundles: substance or sophistry? Anaesthesia. 2006;61:313-315.
Systemic Inflammatory Response Syndrome
The systemic inflammatory response syndrome (SIRS) and multiple organ dysfunction syndrome (MODS) are terms aimed at facilitating standardization of terminology for research into critically ill patients. The systemic inflammatory response is triggered by sepsis, burns, trauma or hypovolaemia, and may be driven by bacterial and endotoxin translocation across an ischaemic, damaged gut (Fig. 7.11).

SIRS is defined as the presence of two or more of the following:
Inflammatory mediators include:
El-Menyar A.A., Davidson B.L. Clinical implications of cytokines in the critical-care unit. Expert Rev Cardiovasc Ther. 2009;7:835-845.
Marik P.E. Total splanchnic resuscitation, SIRS, and MODS. Crit Care Med. 1998;27:257.
Muckart D.J., Bhagwanjee S. American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference definitions of the systemic inflammatory response syndrome and allied disorders in relation to critically injured patients. Crit Care Med. 1997;25:1789-1795.
Webster N.R., Galley H.F. Immunomodulation in the critically ill. Br J Anaesth. 2009;103:70-81.
[/level-membership-for-surgery-category][not-level-membership-for-surgery-category]
Chapter 7 Intensive care
Acute Respiratory Distress Syndrome (ARDS)
Causes
| Direct injury | Indirect injury |
|---|---|
| Pulmonary contusion | Septicaemia |
| Gastric aspiration | Major trauma |
| Fat and amniotic fluid embolus | Cardiopulmonary bypass |
| Infection | Massive blood transfusion |
| Cytotoxic drugs | Prolonged hypotension |
| Smoke inhalation | Hepatic and renal failure |
| Oxygen toxicity | Disseminated intravascular coagulation |
Pathophysiology
Activated neutrophils adhere to endothelial cells and release inflammatory mediators, including oxygen-free radicals and proteases, to cause lung damage. Direct lung damage or endotoxins alone are sufficient to damage endothelial cells with cytokine release and an inflammatory cascade (Fig. 7.1).
Treatment
Treat underlying cause
Other methods of improving oxygenation
and arterial oxygenation. Long-term benefits have not been proven.Secondary infection. High risk of secondary infection reduced with prophylactic antibiotics.
Acutely Ill Patients in Hospital: Recognition of and Response to Acute Illness in Adults in Hospital
National Institute for Clinical Excellence 2007
Guidance
Chan K.P., Stewart T.E., Mehta S. High-frequency oscillatory ventilation for adult patients with ARDS. Chest. 2007;131:1907-1916.
Dernaika T.A., Keddissi J.I., Kinasewitz G.T. Update on ARDS: beyond the low tidal volume. Am J Med Sci. 2009;337:360-367.
Malarkkan N., Snook N.J., Lumb A.B. New aspects of ventilation in acute lung injury. Anaesthesia. 2003;58:647-667.
McLuckie A. High-frequency oscillation in acute respiratory distress syndrome (ARDS). Br J Anaesth. 2004;93:322-323.
Moloney E.D., Griffiths M.J.D. Protective ventilation of patients with acute respiratory distress syndrome. Br J Anaesth. 2004;92:261-270.
NICE. Quick reference guide. Acutely ill patients in hospital. NICE clinical guideline, 2007;50. www.nice.org.uk/nicemedia/pdf/CG50QuickRefGuide.pdf.
Rouby J.-J., Consstantin .J-M., Girardi C.R., et al. Mechanical ventilation in patients with acute respiratory distress syndrome. Anesthesiology. 2004;101:228-234.
Cardiovascular System
Inotropes
If shock persists despite adequate volume replacement and vital organ perfusion is jeopardized, inotropic drugs may be required to improve blood pressure and cardiac output (Table 7.2).
Adrenergic receptor function
α1 receptors activate phospholipase C which cleaves phosphoinositol 4,5-biphosphate (PIP2) to diacylglycerol (DAG) and inositol triphosphate (IP3). DAG activates protein kinase C to release arachidonic acid which increases cGMP synthesis (Fig. 7.2). Activation of β1, β2 and dopamine (D1) receptors triggers the conversion of ATP to cAMP, activating protein kinase C and triggering protein phosphorylation which causes tachycardia and increases contractility (Fig. 7.3).
Pulmonary artery catheters
Indications
Complications
Table 7.3 Complications of pulmonary artery catheter insertion
| Associated with insertion | Associated with catheter presence |
|---|---|
| Pneumothorax/haemothorax | Infection of catheter or site |
| Haematoma | Pulmonary thrombosis/infarct |
| Cardiac arrhythmias | Cardiac arrhythmias |
| Arterial puncture | Valve damage/endocarditis |
| Pulmonary artery perforation | Pulmonary artery erosion |
| Catheter knotting | Thrombocytopenia |
| Cardiac valve damage |
Cardiac output monitoring
Invasive techniques
Non-invasive techniques
American Society of Anesthesiologists Task Force on Pulmonary Artery Catheterization. Practice guidelines for pulmonary artery catheterization. Anesthesiology. 2003;99:988-1014.
Antonelli M., Levy M., Andrews P.J., et al. Hemodynamic monitoring in shock and implications for management. International Consensus Conference. Intensive Care Med. 2007;33:575-590.
Dawson S., Jhanji S., Pears J.R.M. Cardiac output monitoring: basic science and clinical application. Anaesthesia. 2008;63:172-181.
Jhanji S., Dawson J., Pearse R.M. Cardiac output monitoring: basic science and clinical application. Anaesthesia. 2008;63:172-181.
Klein A.A., Snell A., Nashef S.A., et al. The impact of intra-operative transoesophageal echocardiography on cardiac surgical practice. Anaesthesia. 2009;64:947-952.
Moppett I., Shajar M. Transoesophageal echocardiography. BJA CEPD Rev. 2001;1:72-75.
Van Lieshout J.J., Wesseling K.H. Continuous cardiac output by pulse contour analysis? Br J Anaesth. 2001;86:467-469.
Fluid and Electrolyte Balance
The neonate has a greater proportion of body water and in a different distribution than the adult (Fig. 7.5). More fluid is distributed within the extracellular compartment (interstitial and plasma volume) compared with the adult, resulting in a larger volume of distribution for water-soluble drugs. A large proportion of interstitial fluid is excreted within the first few weeks after birth and adult levels are attained by adolescence.
A 70 kg male has about 42 kg of water distributed through three body compartments.
Normal fluid requirements
Postoperative fluid requirements
Intravenous fluids administered perioperatively during minor gynaecological surgery reduce morbidity, particularly nausea and dizziness. However, blood coagulation appears to be accelerated by haemodilution with saline, and in patients undergoing elective abdominal surgery, the incidence of DVT was four times greater than in the fluid-restricted group (Janvrin et al 1980).
Albumin
Benefits of correcting hypoalbuminaemia are unclear. A prospective randomized study of 475 ICU patients comparing albumin and gelatin solutions failed to show any benefit (Stockwell et al 1992). In 70 children with burns, albumin supplementation failed to improve morbidity or mortality (Greenhalgh et al 1995). In septic patients, albumin infusions will only increase COP for a relatively short period. Increased capillary permeability results in >60% of albumin leaving the intravascular compartment within 4 h, potentially worsening oedema.
A controversial systematic review by the Cochrane Group of 23 randomized controlled trials found that the risk of death was 6% greater in the group treated with albumin compared with those receiving crystalloids or no treatment (Cochrane Injuries Group 1998). The Committee on Safety of Medicines now advises doctors to restrict the use of, and take special care when using, human albumin, but states that there is ‘insufficient evidence of harm to warrant withdrawal of albumin’. Hypoalbuminaemia in itself is not an appropriate indication. Risks of hypervolaemia and cardiovascular overload warrant monitoring in patients receiving albumin.
