Integrating technology into clinical practice in neurological rehabilitation*
KATIE BYL, PhD, NANCY N. BYL, PT, MPH, PhD, FAPTA, MARTEN BYL, PhD, BRADLEY W. STOCKERT, PT, PhD, SEBASTIAN SOVERO, MS, CLAYTON D. GABLE, PT, PhD and DARCY A. UMPHRED, PT, PhD, FAPTA
After reading this chapter the student or therapist will be able to:
1. Summarize the need, demand and principles for integrating advanced robotic technology in neurological rehabilitation.
2. Define common terminology used in the field of rehabilitation robotics and technology.
3. Classify the different types of advanced technology used in neurorehabilitation.
a. Rehabilitation robots and assistive technology including:
i. Service robots for movement
ii. Service robots for physical assistance and indoor and outdoor navigation
iii. Nonwearable robotic assistive device for mobility, unweighting, and object manipulation
iv. Wearable robotic assistive device for upper-limb object manipulation
v. Wearable robotic assistive device for lower-limb mobility and gait training
vi. Communication robotics to enable interpersonal interaction
vii. Interactive entertainment robotics for companionship and emotional support
b. Advanced clinical technology including:
i. Virtual reality training systems for improved neural recovery of upper- and lower-limb function
ii. Computerized learning-based gaming systems for home training of individuals with physical disabilities and memory impairments
iii. Computerized patient simulators for teaching clinical diagnoses and intervention strategies to medical professionals
iv. Computer technology for teaching home exercise programs to patients
4. Use the guidelines for integrating robotics and assistive technology into a patient’s rehabilitation program.
5. Summarize the challenges and basic engineering principles involved in creating rehabilitation robotics and interfacing with advanced technology to help individuals to design:
a. Robots that operate independently
b. Controllers, actuators, and sensors required for service and assistive rehabilitation robots
c. Human interfaces (physical, sensory physical, cognitive, and brain machine)
d. User-friendly interfaces and controllers to maximize kinematics (e.g., force, velocity, timing)
e. Rehabilitation robotics based on the materials and control technology currently available
f. Safe robotics for rehabilitation
6. Discuss the benefits of performing a cost-effectiveness analysis when considering the application of robotic technology in rehabilitation.
7. Describe the challenges of commercializing robotic devices.
8. Discuss the future of advanced technology and rehabilitation.
Introduction to the application of robotics and technology in rehabilitation
General overview
The objective of rehabilitation technology is to empower clinicians and individuals to take responsibility and control of the environment, facilitate physical and cognitive recovery, and comply with learning-based practice to drive neural adaptation and neural reorganization. The principles underlying technology and rehabilitation are summarized in Box 38-1. Since the early 1990s, medical science has been able to minimize damage to the nervous system postinjury. It is known that the central nervous system (CNS) possesses the potential for spontaneous healing and recovery. Learning-based sensory and motor training can be used to drive recovery of function. Rehabilitation robotics are a logical addition to supervised, one-on-one therapeutic interventions.1–9
BOX 38-1  PRINCIPLES SUPPORTING ADVANCED TECHNOLOGY AND REHABILITATION ROBOTICS IN NEUROREHABILITATION
PRINCIPLES SUPPORTING ADVANCED TECHNOLOGY AND REHABILITATION ROBOTICS IN NEUROREHABILITATION
Goals for advanced technology and rehabilitation robotics include the following:
A Indirectly augmenting functional independence of individuals with impairments by:
1. performing mobility tasks for individuals at the home (e.g., using automatic motorized wheelchairs to move individuals from room to room; transitioning individuals from bed to chair and from chair to standing; moving patients who are standing; smart houses; calling for help)
2. minimizing the need for assistance from another individual
3. performing functional activities of daily living (ADLs; e.g., getting objects, cooking food, doing dishes, bathing, transferring)
4. helping perform difficult or repetitive tasks at work (e.g., assembly line tasks; lifting and moving heavy objects)
B Directly improving human motor skill capabilities of individuals with impairments to enable them to:
The objectives of assistive rehabilitation robotic devices need to be clearly defined in terms of:
A unweighting a limb to reduce patient effort required for movement
B actively canceling mechanical limitations on movement of the patient and robot arm dynamics (e.g., friction, inertia, and weight under gravity)
C gently and progressively moving a limb to assist patient effort to perform a task
D stabilizing a joint to enable a patient to produce a controlled movement
E assisting the patient to improve the accuracy and quality of a movement
Robotic technology for rehabilitation needs to be defined by:
A location of the control system relative to the patient (controlled at a distance from the user [e.g., Web, Skype]), controlled in proximity to the user [e.g., by a therapist or engineer], or controlled by the user [e.g., wearable device or interface])
B environmental connection of the device and the patient (fixed to a nonmobile surface [e.g., wall], attached to a mobile platform [e.g., wheelchair], freely mobile with the patient [wearable])
C type of control system (e.g., joystick, sensor, breath)
D type of interface (physical, sensory, cognitive, brain)
E type of anatomical connection (e.g., by end effector only, end effector and multiple points of attachments with serial links or temporal links)
Robotic technology can provide service, unweighting, passive assistance, active assistance, variable and on-demand assistance, or a combination of service and assistance.10 Computerized and robotic technology provides the foundation for patients to practice and attend to purposeful, goal-oriented, progressive tasks spaced over time. This technology can also minimize the risk of injury during retraining. Robotic interfaces, actuators, and controllers can convert sensory, physical, and cognitive signals to control robots, permit perception of spatial relationships, mobilize individuals in space, assist in object manipulation, provide emotional support, and allow individuals to call for help and communicate with others. In addition, through creative virtual training environments and gaming technology, patients can improve memory, motor skills, and movement quality. In addition, patient simulators can help medical professionals learn diagnostic processes, treatment interventions, and manual techniques. Computer-assisted technology can also improve our ability to teach home exercise programs to patients. Over the next 10 years, robotic technology will expand the opportunities for clinicians to assist patients to achieve maximum independence and quality of life with less dependence on others.
History supporting the use of technology in neurological rehabilitation
The idea of interfacing technology with rehabilitation was introduced into practice by George J. Kelin in the 1940s. Kelin was a productive inventor from Canada who invented the power wheelchair for patients with quadriplegia, the microsurgical staple gun, and a wide range of industrial gearing systems. He also contributed to internationally important innovations in aviation and space technology. During the early 1970s, a new field emerged known as mechatronics, which combines mechanical, electrical, and control engineering design principles to produce a diverse range of useful practical devices.11,12 The science of biomechatronics then developed as a unique engineering discipline responsible for integrating neuromusculoskeletal appliances with biological systems to control and facilitate human-machine interactions as well as developing interfaces, sensors, actuators, and energy supplies to create functional devices for human use.13
The first conference on rehabilitation robotics was held in 1990. There are now multiple conferences each year on rehabilitation robotics. In 1999 the Robotics and Automation Society created the Rehabilitation Robotics Technical Committee to improve definitions and understanding about rehabilitation and assistive robotics.14 The scope of this technical committee has been recently specified as rehabilitation and assistive robotics. This modification is the direct outcome of the scientific progress and maturity reached in this broad research area. The goal of rehabilitation robotics is to investigate the application of robotics to therapeutic procedures for achieving the best possible motor, cognitive, and functional recovery for persons with impairments associated with aging, disease, or trauma (e.g., stroke, neuromotor disorders, brain trauma, orthopedic trauma, cognitive disease).
Some clinicians have been skeptical of robotics in rehabilitation. Some health care providers worry that robots will replace therapists; others worry that robots are unsafe.8 However, researchers have persisted in developing innovative hardware, new control strategies, improved compliance, and feed-forward and adaptive control systems, as well as computerized modeling. In addition, new assistive, wearable robotic arm devices have been developed (e.g., MIT-Manus, the MIME, the ARM, and the iARM) to more carefully outline and address the engineering challenges related to what the robot can do, the logical physical targets for active assistance, and the joints and the types of movements that can safely be assisted.
The field of rehabilitation robotics is still considered to be in its infancy. However, with the increasing demand for effective rehabilitative strategies, many new and exciting innovations are being developed. There are many robotic systems in various stages of research and development, but only a few are commercially available. Improvements in engineering, materials, human physical interfaces, software, and robotic designs will require constant analysis and adjustment in the future. It is projected that the market for personal robotic devices will be worth $15 billion by the year 2015.15,16 The challenges of robotic engineering are broad. Clinicians will need to participate in research to help document cost-effective outcomes as well as to develop efficient screening criteria to match patient needs with available robotic devices. One of these challenges will be to bridge the gap between the mechanical attributes of robotic sensors, actuators, controls, microprocessors, force, velocity, friction, unweighting, pressure tolerance, software design, and flexibility with the human limb, brain, and nervous system. Important issues related to safety, materials, technology, and the quality of matching machine and human movements must constantly be considered. These engineering issues are discussed later in this chapter.
Classification of rehabilitation robots
General principles
There is a variety of ways to classify computerized technology for rehabilitation. For this chapter, we will group robotic technology first in terms of how robotics are used with or by the client relative to rehabilitation. This classification system is summarized in Figure 38-1 and Box 38-2. Rehabilitation technology can be further classified by a variety of variables summarized in Box 38-3. Rehabilitation robotics can also be classified by type of interface used. Some classification systems classify technology by multiple parameters.
















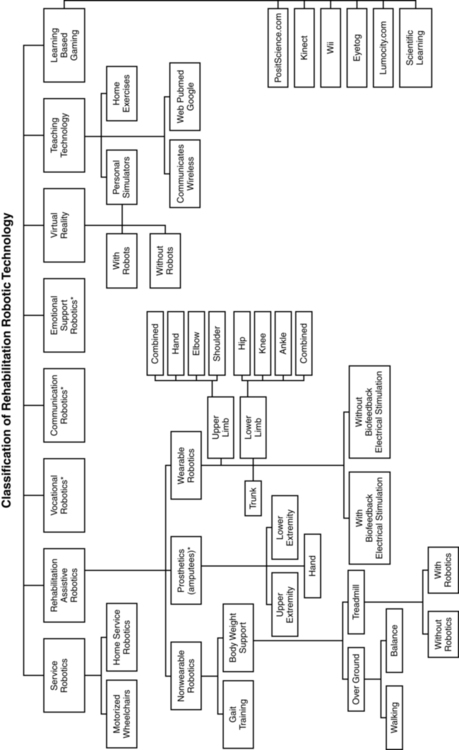

Service robots usually focus on task performance, movement assistance, and stability. These devices can be fixed, can be movable, or can be attached to a wheelchair (Box 38-4). Assistive robotic devices help patients perform a task with direct or indirect assistance. Some of the assistive robotics are nonwearable but assist through unweighting or movement assistance (Box 38-5). Wearable robotics are specifically designed to be worn by patients to assist movements. These are designed for the upper or lower limb (Box 38-6). There are some new assistive training devices for the spine such as the Valedo Shape, Valedo Motion, and Hocoma devices (Figure 38-2). Prosthetic devices help patients maintain function despite the loss of a limb. Vocational robotics can enhance performance at work either in terms of repetitive motions or high-force task production that would otherwise be dangerous to humans. Communication robotic devices are designed to improve communication potential for subjects who cannot adequately speak or hear. Emotional support robotics are designed to provide emotional support for isolated individuals at home.






BOX 38-5  TYPES OF NONWEARABLE ASSISTIVE ROBOTIC DEVICES
TYPES OF NONWEARABLE ASSISTIVE ROBOTIC DEVICES
 Body-weight–supported mobile walking aids
Body-weight–supported mobile walking aids
 Robotic devices for physical support (indoors, outdoors)
Robotic devices for physical support (indoors, outdoors)
 Robotic devices for physical support, unweighting, and mechanical stepping in place
Robotic devices for physical support, unweighting, and mechanical stepping in place
 Robotic devices for unweighting and controlled destabilization
Robotic devices for unweighting and controlled destabilization
 Robotic devices for unweighting and gait training
Robotic devices for unweighting and gait training
 Robotic devices for unweighting and robotic stepping on a treadmill
Robotic devices for unweighting and robotic stepping on a treadmill




 ed (
ed ( pper •imb)
pper •imb)








VR training technology (with and without robotics) provides the opportunity to simulate simple and complex environmental and clinical situations to facilitate learning (Box 38-7). Game-oriented computerized learning systems are currently popular for fun and recreation, but they can also facilitate memory as well as sensory and motor skill development. Finally, computerized technology can also enhance teaching home exercises to patients.
BOX 38-7  EXAMPLES OF HOW VIRTUAL REALITY CAN ASSIST LEARNING
EXAMPLES OF HOW VIRTUAL REALITY CAN ASSIST LEARNING




In this chapter, we will not address prosthetics for amputees, vocational robotics, communication robotics, emotional support robotics, or socially assistive devices,17,18 as these areas are considered specialty oriented and may or may not be included in traditional neurorehabilitation programs coordinated by physical or occupational therapists. However, information about the impact of the sound of the robot voice on patient motivation and compliance may be relevant to effectiveness. It is also important to acknowledge there are a number of motorized chairs, lifts, and walkers available that can be used to transition a patient from sitting to standing, or provide unweighting while walking or working on balance. Examples can be found in Box 38-8. Many of these systems are electromechanical systems controlled by the patient or the therapist. These devices are not usually programmable and are not classified as “rehabilitation robotics” or “advanced technology.” However, these types of devices are very beneficial for helping patients maintain walking and training to improve safety and quality of gait at home and with supervision. It is important for therapists to be sure these types of assistive devices have been integrated into a patient’s rehabilitation program and at home before recommending more sophisticated technology.


 ’ Go wa•ker
’ Go wa•ker


Description of robotic systems by type
Service robotic systems that provide movement assistance
Service robotics assist individuals with severe disabilities. Most commonly, the robot performs everyday activities (e.g., assisting with eating, drinking, object replacing, ambulating). There are three main types of schemes: desktop-mounted robots, wheelchair-mounted robots, and mobile autonomous robots. In general, these robots are used in the home, are interconnected to a variety of control systems, and are programmed to the environment and consequently are not very portable.19–21
Several examples of service robotics are described in Box 38-9.22–30 A major issue is patient control options for service robotic devices. For example, through the use of headpieces on robotic devices, information can be detected from flexion and extension, rotation, and side bending of the head to operate wheelchairs, TV sets, telephones, doors, and security systems. There are also some new interfaces that are sensitive to facial movements and optoelectronic detection of light-reflective head movements.31 Other interfaces are sensitive to eye movements or use voice recognition, brain control,32,33 and gesture recognition.34 These interfaces not only may allow control of the robot but also may be applied to move a limb or perform a task.
BOX 38-9  SUMMARY OF SERVICE ROBOTICS
SUMMARY OF SERVICE ROBOTICS
I. Fixed upper-extremity service robotic devices
A The earliest robots were fixed-site robots.
B Fixed robotics were located in a nonmovable workstation.
1. The arm was preprogrammed to carry out selected routines which the user selected by pressing appropriate buttons (e.g., Seamone and Schmeisser at Johns Hopkins University, l974).
2. These workstations led to early Desktop Vocational Assistive Robots
C Stanford University researchers, Boeing, and researchers responsible for several advances in France made significant improvements, particularly in integrating existing robotic systems.
D Later, special manipulators were constructed to better fit the environment and the task.
E The most well known systems for feeding were the Handy 1, My Spoon, and Neater Eater.22
F Today, these devices have been advanced with powered programmable devices (devices can provide maximum control for those with minimal voluntary ability and assistance for individuals who are trying to retrain the arm to work in a functional task).
II. Mobile service upper-limb robots
A Mobile service upper-limb robots are actually mechanical slaves. They are instructed to perform tasks.
B The technology must be adequate to operate autonomously.
C These units are expensive both in development and maintenance and usually require an engineer to set them up in the house and maintain their function over time.
1. The best known was developed in California at Stanford (the MoVAR system).23
2. This has a mobile base and a console to give feedback to the user to improve control.
3. The HelpMate robot is another mobile service robot that a disabled person can use to carry things from one place to another. If there is a cluttered environment within the home, that external environment negates the practical use of this robot.
4. The KARES II robot system24 uses a visual server to help provide assistance with movement (e.g., an eye mouse and a haptic suit with the arm mounted on a remote-controlled mobile base).
5. The Wessex robot allows different tasks to be performed in different rooms.
III. Wheelchair-mounted upper-extremity manipulators
A Wheelchair-mounted manipulators were first designed at the VA Prosthetics Center in New York (1984).
1. This sophisticated wheelchair-mounted manipulator is able to reach from the floor to the ceiling.
2. It has 7 degrees of freedom and a gripper hand.
3. This device may be sold to a rehabilitation facility to enable training of multiple users at that site. It is also sold to individual users. It is relatively expensive.
B The Raptor25 was produced at a lower cost (only 4 degrees of freedom).
C Exact Dynamics has also created a robotic manipulator (iARM) that is designed to help provide independence to people with severe disabilities.
D Exact Dynamics also produces the Dynamic Arm Support (DAS), which compensates for the forces of gravity, making the arm practically weightless. These devices are currently being used in rehabilitation settings for training and for research.
IV. Automatically guided wheelchairs (agws)
A Powered wheelchairs can have autonomous intelligence systems attached.
B AGWs are service rehabilitation robots intended to move the individual with severe disability.
C Computer sensing devices can be set up to handle emergencies and assist with task performance.
D The robot must receive instruction about the destination point.
1. These work best in a fixed, predictable environment and operate on an information decoding system whereby sensors identify the position and compare that position to the destination.
2. The algorithm must create a collision-free path from the starting point to a target.
3. Some robotic devices detect location and perform object avoidance behaviors through the use of ceiling-mounted or doorframe-mounted cameras.
4. In some cases the user may be able to modify the environmental situation by programming in new obstacles.
V. Rehabilitation service robots: smart house design
A For individuals with physical disabilities and older individuals, these smart devices allow residents to live independently with minimal or no human assistance.
B There are a number of smart devices that can be installed in the house that are linked to one another to process information from the inhabitant to make decisions and take actions in case of emergency.
C Smart house designs continue to be an area of development, particularly with the increasing number of aged individuals who are no longer able to manage independently.
1. One example is the Robotic Room developed at the Sato Laboratory of the Research Center for Advanced Science and Technology in the University of Tokyo.26
2. The Robotic Room consists of a ceiling-mounted robot arm (long-reach manipulator) and an intelligent bed with pressure sensors for monitoring the person’s posture.
a. Modules monitor respiration without attachments.
b. Cameras detect positions of the ends of the quilt on the bed.
c. There is a second robot that is mobile to perform transportation tasks. The cameras on the ceiling detect robot positions.
d. The interface of the robot consists of three ceiling-mounted video cameras to detect orientation of the user’s hand. When the user points at the robot, the television, curtains, and so on will be controlled.
VI. Functional integration of multiple robots in the intelligent home environment
A In the intelligent home environment, there are additional rehabilitation robotics designed to work with home-installed devices.
B Placed in the correct arrangement, these robotic devices are controlled in a coordinated manner.
1. The M3S (multiple master–multiple slave) is a communication robot installed in the home.
2. This robotic system started with the TIDE Project27–29 and has set the standard for this type of robots.
3. Users can assemble a specific complete modular system.
4. In case of emergency, the user can halt the operation of the whole system (“dead man switch”).
5. The ICAN Project (Integrated Control for All Needs) developed the functional integration aspects of the system.23
6. The main objective is to propose an optimal control over all home-installed devices by a single interface device (e.g., joystick or switch input).
7. ICAN is a collaborative project in Europe and continues to receive government support.30
Assistive robotics
Nonwearable assistive robotic devices.
Types of nonwearable assistive robotic devices.
There is a variety of nonwearable assistive robotic devices. Some of these nonwearable assistive robotic devices are summarized in Box 38-10.35–43 This group of robotic devices primarily includes powered wheelchairs with autonomous intelligence, body-weight–supported mobile walking aids, robots for body support with indoor and outdoor navigation, hands-off service robotic devices, and body-weight–supported treadmill systems (BWSTSs) with and without robotics.37,41–45
BOX 38-10  NONWEARABLE ASSISTIVE ROBOTIC DEVICES FOR GAIT TRAINING
NONWEARABLE ASSISTIVE ROBOTIC DEVICES FOR GAIT TRAINING
I. Body-weight–supported mobile walking aids
A Newly designed rehabilitation robotic systems can function as walking aids to help those who cannot walk independently.
B Some mobile walking aids can walk the client, but others can also be used for training the patient to walk.
1. There are several electric motor-based gait rehabilitation systems.
2. Generally, gait rehabilitation systems include a robotic manipulator, a mobile platform, and a sensor system.
3. The robotic manipulator controls the amount of body-weight support.
4. The robot is mounted on a mobile platform that not only can support the user’s weight but can be adjusted to the height of the subject and provide stability when walking.
5. The robot has sensors to detect the status of the user (direction and velocity).
6. The mobile platform moves the whole system according to the subject’s motion with objects in the way of the moving platform detected by ultrasonic sensors on the front of the system.43
a. The mobile platform can vary from having a carlike design to having a mobile base with driving and steering wheels and differential driving mobile bases.
b. The front-wheel-drive carlike model has a complex mechanical design and can be very expensive.
c. The synchronous driving and steering mechanisms are complex but can approximate human walking, especially when the path is not linear.
d. Differential driving mechanisms require two independent driving wheels.
e. The mechanical architecture is simple and practical to implement but may require more maintenance.
f. There are training and following modes.
g. The challenge is to have sensors that can control stop and go of the user.
h. The supervisor can push an emergency stop button, but if the user is generally weak and does not have adequate balance reaction, the patient could fall when the mobile unit stops suddenly.
i. Example: the gait rehabilitation system:
(a) Used to study the impact of unweighting on gait parameters and patient exertion and heart rate.37
(b) Researchers have demonstrated that with increasing amounts of unweighting, there is an increase in single leg support and a decrease in double leg support, in terms of the percentage of time a given leg contacts the ground during steady-state walking.
(1) At 0% unweighting, single leg stance was 34.5%.
(2) At 20% unweighting, single leg stance was 38%, with 23% on both limbs.
(3) At 40% body unweighting, single leg stance was 42.5%, and 17.5% of time included bilateral support.
(c) With increased unweighting and comfortable walking speed, there is a decrease in heart rate.
C If the device is primarily used to facilitate standing to prevent contractures and skin ulcers, it may be classified as a stander rather than a walking aide.
II. Robots for physical support
1. These devices assist users with limb and trunk weakness and visual impairments; usually the patients are older.
2. These machines usually have a motorized base to give physical support to the user.
3. The robot control system identifies its specific location and puts out voice synthesized navigation instructions or warnings about obstacles on the intended routes.
4. The robot automatically detects the user intention regarding walking speed and direction of movement.
5. Examples include the HITOMI,38 the PAM-AID,39 and the WHERE (walking and moving helper robot system).37
B Indoor and outdoor navigation
1. These devices provide physical support for unweighting, harness or robotically controlled protection from falling, and the ability to step.
2. The robot protects against falling when the end-range body sway has been exceeded.
3. These devices are best for improving postural righting reactions without falling.
C Unweighting with robotic-controlled stepping
1. These devices can include harness support and unweighting while the user stands on an electromechanical platform system.
2. The feet are attached to assistive computerized devices that force stepping of the feet.
3. Training is done on the device (e.g., electromechanical gait trainer developed by Hesse).
4. With practice in stepping, the goal is to improve efficiency and effectiveness of walking.
5. Studies with this device confirm it is safe and there are improved outcomes as measured by increased walking speed and endurance.
D Unweighting with robotic-controlled destabilization
1. One device that has been tested at the University of Chicago is the KineAssist (IMAGE).40 (See Figure 38-6.)
2. The KineAssist is a robotic gait training device that emphasizes balance recovery training during gait training.
3. The goal is to provide partial body-weight support and postural control on the torso while the patient walks over ground.
a. This device is on a mobile, multidirectional base that allows the patient to walk over ground, indoors or outdoors.
b. The trunk and pelvis are free to move, the legs are accessible, and the arms are free.
c. A servomotor follows the patient in forward, rotation, and sideways walking.
d. It has a robotic arm that is linked to the patient’s trunk.
e. The robotic arm can be set to allow the patient to move easily and even exceed the limit of stability.
f. The robot can also be programmed to specifically interfere with stability.
g. The patient can lose balance and “fall,” but the robotic arm will stop the fall after a defined range.
h. The patient can experience what is needed to keep from falling when the limit of stability has been reached.
i. With practice the patient can improve postural righting and balance.
A These are devices that can be placed on the less affected side to restrict motion of a limb.
B The objective is to force the patient to use the affected limb (similar to constraint-induced therapy in which the least-affected limb is constrained with a mitt or a cast; see Chapter 9).
C Usually the robot is programmed to perform specific tasks with the patient assisting.
D The robot could give feedback by nodding, talking in a synthesized voice, or using a prerecorded friendly human voice with humor and engagement that could be matched to some extent to the patient’s personality.
E Patients appear to perform better when they receive a robot voice for feedback and the robot personality is matched to the patient.
IV. Body-weight–supported gait training systems
A Without computerized assistance for stepping
1. Body-weight–supported gait training systems are designed to unweight the body to enable the patient to walk more easily.
2. The purpose of unweighting is to decrease ground reaction forces, protect against falling, improve balance, and improve walking speed over ground (see Table 38-4).
3. Most of these devices integrate self-regulated stepping by stimulating the automatic stretch stimulus to activate the pattern generator for stepping at the spinal cord level.
4. With unweighting, it is possible to maintain physical activity while undergoing healing and recovery.
5. Progressive unweighting and reweighting may also be important for maintaining bone mineralization during healing.
6. Unweighting may also make it possible for patients to perform more complex tasks such as one-footed balance, end range reaching without falling, and coordinated movement patterns such as skipping, dancing, ice skating, and roller skating without the risk of falling.
a. Patients can slowly build up endurance and strength as well as perform tasks that are difficult when fully weighted (e.g., rising on toes, squatting, jumping, skipping).
b. When unweighting is used over the treadmill, it is possible to increase the treadmill speed so the individual who is training can achieve higher speeds of walking or running.
8. A variety of unweighting systems are available for gait training. Most use a harness system; however, in 2011 new unweighting systems that use a harness and a leg system, air, or a bike seat were introduced.
a. Some emphasize walking over a treadmill and some over ground.
b. Some emphasize balance training and some emphasize gait training.
c. Most unweighting systems are comfortable at up to 20% to 30% of unweighting.
d. Some body-weight–support systems can comfortably unweight the body up to 80% (AlterG), and some 100% (e.g., GlideTrak, Gait Trainer).
i. In 2008, the AlterG air-distributed unweighting treadmill systems were approved by the U.S. Food and Drug Administration (FDA) for physical rehabilitation and gait training.
(a) The patient stands on the treadmill in an enclosed waist-high pressurized bag air-chamber.
(b) During use, pressure inside the chamber is increased until the pressure difference across the waist seal generates an upward “lifting” force, evenly distributed to the lower body to counter gravitational body weight.
(c) As pressure within the chamber is increased, a greater proportion of the patient’s body weight is supported (a range of 0% to 80% for patients weighing 140 to 300 pounds).14
(d) The unit can be ordered with portholes to allow the therapist to reach into the bag to assist the patient.
ii. In 2010 the concept of a bicycle was used for unweighting.
(a) The GlideCycle unweights the patient by supporting the patient through the pelvis on a posted seat similar to a bicycle with anterior bar support against the ilium.
(b) The patient is essentially standing in a cone of support to stride with the legs.
(c) This system can be used on a treadmill or over ground. The legs are free to move in a stride-type fashion.
(d) When the patient swings the arms, an increased demand is placed on balance.
(e) Stepping the legs can be easily facilitated by a therapist.
(f) When the unweighting is performed over ground on a two-wheel or four-wheel bicycle, the individual can be outside and enjoy the terrain, still unweighted.
B Body-unweighting treadmill systems with computer assistance for stepping and walking
1. Some body unweighting systems include a robot to assist with stepping.
a. The Lokomat (Hocoma) is a body-unweighting treadmill system that uses a harness for unweighting, suspending the patient over a treadmill.
i. An exoskeleton, robotic manipulator is attached to the patient’s legs with many sensors to detect the status of the user and step the legs.
ii. With linear potentiometers attached, the user’s walking direction and velocity are analyzed, and then parameters are computer generated to assist the patient in walking.
(a) Walking is facilitated by setting the speed of the treadmill and setting the parameters of leg movement.
(b) Use of the device is referred to as “robot-assisted walking therapy” and involves passive movement.
(c) At the early stage of spinal cord injury, the goal is to stimulate neural adaptation and recovery.
(d) In the late stage of healing after spinal cord injury, the objective is to facilitate good metabolism, prevent contractures, decrease bone demineralization, and facilitate well-being.
2. Other laboratory model robotic gait trainers use a system of cuffs and straps to help walk the legs.41,42
a. One system is a simple strap system (ARTHuR).
b. Another system includes a combination of straps and computerized control systems (PAM and POGO).
c. The KNEXO is a bilateral lower-limb robot-assisted exoskeleton developed by Pieter Beyl in Brussels.
i. This includes an evaluation platform and a gait training device.
ii. It has a high-force pleated pneumatic artificial muscle (PPAM) system to enable full knee support during treadmill walking.
iii. It has a zero torque mode for unassisted walking and reference knee pattern recording.
iv. It has a tunable assistive mode with safe interaction with human movement. Stepping is facilitated over a treadmill.
i. Novel system for gait rehabilitation
iii. Purpose is to restore posture and gait functions
iv. Provides partial body-weight support
v. Supports patient to autonomously perform gait training
e. Passive gravity balancing leg orthosis (University of Delaware)35,36
ii. Has a hip linear actuator.
iii. Spring-loaded winch to support device weight.
iv. Walker used to support the device.
v. Used over the treadmill but will be used over ground.
vi. Load cell on hip linear-actuator.
viii. The orthosis is connected to a walker, and its trunk has four degrees of freedom with respect to the walker (vertical and lateral translation, rotation about vertical axis and horizontal axis perpendicular to sagittal plane).
ix. Hip joint has two degrees of freedom with respect to the trunk, one in the sagittal plane and the other for abduction-adduction motion.
x. Knee has one degree of freedom with respect to the thigh segment.
Purpose of nonwearable assistive robotic devices.
Nonwearable assistive robotic devices were designed primarily to facilitate mobility and gait training. More specifically, body-weight–supported gait training systems were initially designed to unweight the body, decrease ground reaction forces (GRFs), and protect against falling (Figure 38-3). Under these assisted conditions, it is easier for patients to achieve intense levels of exercise such as walking, skipping, and running with less pain and less trauma to the joints.46 These systems also allow runners to exceed the speed of overground running while being protected from falling.47 Unweighting also allows patients to increase their heart rate more slowly while running or jogging at a higher speed.47 For patients with spinal cord injuries, body unweighting over a treadmill was a translation of basic science findings to clinical practice. In animal studies, walking ability could be restored after induced spinal cord injury by facilitating the spinal generator for stepping through movement of the treadmill belt.48–50 Through unweighting, it is also possible to maintain metabolic activity while allowing healing and recovery after joint inflammation, muscle injuries, degenerative joint conditions, bone fractures, surgical repairs, joint replacements, osteoporosis, stroke, or head trauma. Most of the research on bone density is based on studies involving patients with spinal cord injuries. In these studies, walking on a BWSTS does not significantly increase bone density. However, those who walk on the BWSTS lose less bone density than those who do not exercise on the treadmill.51,52 On the other hand, although body-weight–supported treadmill training (BWSTT) may not necessarily increase bone density, particularly in patients with spinal cord injuries, exercise (with or without BWSTT) can increase muscle mass and/or prevent atrophy. On the other hand, in one study the use of shorter, frequent mechanical loading sessions was correlated with enhanced bone mass.53 More research is needed to determine the time and frequency of standing and walking exercises and their beneficial effects on bone density.54


Key features of unweighting.
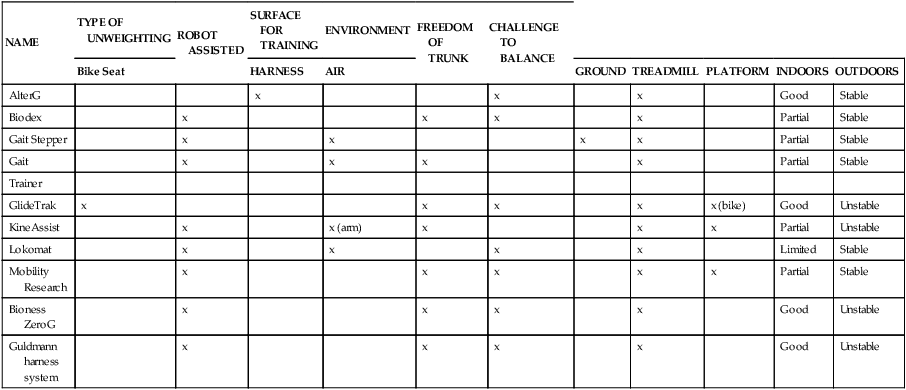
A key feature of BWSTT is the degree, comfort, and convenience of adjustable support.55 Whereas harness systems are the most commonly used for unweighting, when high levels of body support are needed or patients are jogging, these harnesses can be uncomfortable and cause pressure chaffing. This has led to the development of new body-weight–support systems such as the AlterG trainer (Figure 38-4), which uses a lower-body air distribution system, or the GlideTrak and Glide Cycle, which use a suspended bicycle seat–type unweighting system (Figure 38-5). The movement of the treadmill support surface provides an automatic stretch stimulus for the individual to step. In addition, the speed can be modified to stimulate faster or slower lower-extremity movements, which is very beneficial for individuals who need to vary the rate and responsiveness of their motor movements, such as clients with Parkinson disease, aging adults, or individuals with balance impairments. See Table 38-1 for a summary of the characteristics of some of the current unweighting systems.
TABLE 38-1 
NONWEARABLE ASSISTIVE UNWEIGHTING GAIT TRAINING SYSTEMS
| NAME | TYPE OF UNWEIGHTING | ROBOT ASSISTED | SURFACE FOR TRAINING | ENVIRONMENT | FREEDOM OF TRUNK | CHALLENGE TO BALANCE | |||||
| Bike Seat | HARNESS | AIR | GROUND | TREADMILL | PLATFORM | INDOORS | OUTDOORS | ||||
| AlterG | x | x | x | Good | Stable | ||||||
| Biodex | x | x | x | x | Partial | Stable | |||||
| Gait Stepper | x | x | x | x | Partial | Stable | |||||
| Gait | x | x | x | x | Partial | Stable | |||||
| Trainer | |||||||||||
| GlideTrak | x | x | x | x | x (bike) | Good | Unstable | ||||
| KineAssist | x | x (arm) | x | x | x | Partial | Unstable | ||||
| Lokomat | x | x | x | x | Limited | Stable | |||||
| Mobility Research | x | x | x | x | x | Partial | Stable | ||||
| Bioness ZeroG | x | x | x | x | Good | Unstable | |||||
| Guldmann harness system | x | x | x | x | Good | Unstable |





Effectiveness of body-unweighting treadmill training.
Various biomechanical studies have been done to confirm the parameters of unweighting. After use of early lower-body positive pressure support (LBPPS) prototypes, Grabowski46,47 reported that GRFs were reduced while metabolic power demands were maintained during running. Individuals could achieve faster running speeds when under conditions of unweighting. With slow-speed running on the LBPPS (1.0 to 1.5 mph), it is possible to reduce GRFs by 50% when the body is unweighted to 27% to 48% of normal body weight. At faster speeds (3 to 5 m/s; 6.6 to 11 mph), individuals must be unweighted to 25% of their body weight to maintain a GRF similar to that during walking over ground.
During progressive levels of unweighting, Ruckstuhl55 compared cardiorespiratory performance, gait parameters, and comfort between a laboratory prototype device similar to the LBPPS AlterG trainer and a traditional harness BWSTS. Subjects reported significantly greater comfort using the AlterG trainer and greater tolerance for high unloading. Subjects had significantly lower heart rates when training on the LBPPS versus the harness-based body support system. Other clinical studies have been carried out to confirm the benefits of body unweighting for patients with neurological problems (Box 38-11).

Patients who make the greater gains in gait speed after BWSTT (e.g., 0.08 m/s) also have greater increases in terminal stance hip extension angle and hip flexion power (product of net joint moment and angular velocity) and higher intensity of muscle firing of the soleus.77
The outcomes studies on BWSTT (in patients after stroke, after spinal cord injury, and with Parkinson disease) have generally positive findings. BWSTT enhances gait speed, endurance, and potentially quality.56–58 It is important to force patients to walk at community-level velocities of at least 0.8 m/s (faster than 2.0 mph).59–63 With forced intensity, patients are more likely to achieve physiological and possibly neuroprotective benefits.64,65 For those who make the greatest gains, the improvement has been noted as increased single-limb support, particularly on the most affected limb of individuals after stroke.66 Although there are positive mobility benefits of BWSTT for patients with spinal cord injuries,58,59,67–73 guidelines still have not been generated regarding the best parameters for training (e.g., speed, amount of unweighting, time of intervention). Furthermore, one randomized clinical trial found that intense task-specific gait training over ground was equally as effective as intense body-weight–supported gait training for patients after stroke and after spinal cord injury.74 In another study, BWSTT produced similar gains in mobility compared with locomotor training at home.56 However, there were more falls in those patients who were started on locomotor training early rather than late. In addition, although the outcomes of improved gait performance are similar for BWSTT and aggressive bracing-assisted walking over ground for patients poststroke, the patients with the most severe impairments made the greatest gains with BWSTT.75 Other researchers have reported statistically significant gains in balance, balance confidence, and quality of life after chronic poststroke patients were trained on a BWSTS. However, over the long term the gains were not necessarily considered to meet the criteria for minimal detectable change.76 It appears that the gains in speed after BWSTT should be 0.16 m/s to achieve a minimal clinically important difference.77 Furthermore, there may be additional training activities that can be done to increase the effectiveness of BWSTT, such as VR training,78 electrical stimulation,79 constraint-induced therapy and/or robotics,70 or dual-task learning-based training.80
One BWSTS device allows the individual to walk overground while having one arm attached to the apparatus. The KineAssist gait trainer–destabilizer is an example of this type of body-supported gait trainer (Figure 38-6). Its primary function is to retrain balance to prevent falling. It is considered a BWSTS because the attached arm perturbs the individual while walking and can also provide some support. It perturbs the individual to fall and then catches the individual before he or she falls to the ground.40



Key elements of wearable assistive robotic devices.
Two major issues in wearable robotic devices are safety and dependability. A third major issue is the quality of the interface with the patient and the control of the assistive robotic device. In designing a wearable robotic device, biological principles must be followed. It is important for the robot to be adaptable with minimal weight, muscle fatigue, and energy consumption. In addition, there should be minimal damage imposed on the tissues while the biological systems have high functionality. The extremities can be used to perform multiple tasks, and the redundancy of the joints and degrees of freedom (shoulder, elbow, and wrist) allow human subjects to perform tasks in a variety of ways, creating high functionality. The robot must be adaptable, have minimal weight, be slim, create minimal muscle fatigue, conserve energy, and be easy to control. In addition, there should be minimal damage imposed on the tissues while the biological systems have high functionality. Consistent with biomechanical function of the upper limb, the upper limb must be able to perform multiple tasks with redundancy of the joints and degrees of freedom from the shoulder to the elbow to the wrist. This redundancy, integrated within different environments, provides the opportunity for variation in movement, high functionality, and minimum energy costs.81
Classification of wearable assistive robotic devices.
Some common types of wearable assistive devices are summarized in Box 38-1210,11,82–114 for the upper extremities (Figure 38-7) and Box 38-1310,11,35,42,115–121 for the lower extremities (Figure 38-8). In general, they are divided into three categories of wearable robots: single-task robots, workstation robots, and wheelchair-mounted manipulators (see Figure 38-7). They can also be classified by whether they use neuromuscular stimulation or biofeedback to assist the movement (Figure 38-9). Some patients use these wearable assistive robotics for training and recovery. Those who have reached a plateau in recovery may continue to use these assistive robotic devices for ongoing functional assistance and safety.
BOX 38-12  WEARABLE ASSISTIVE ROBOTICS FOR THE UPPER LIMB
WEARABLE ASSISTIVE ROBOTICS FOR THE UPPER LIMB
I. Wearable assistive robotic devices: fixed, attached to wheelchair, or mobile83
A Workstation assistive robots (fixed site)
1. Manipulator fixed to a wall or a surface.
2. Manipulator may be able to move in different paths.
3. Control system has information about the objects in the immediate environment.
5. Some are preprogrammed to perform functions for the user.
a. DeVAR (Desktop Vocational Assistive Robot).
b. RTX, Tim Jones, United Kingdom, 1985; paved the way for rehabilitation robotics
c. RAID, Stanford University Telematics for the Integration of Disabled and Elderly people (TIDE)
d. Handy 1 (Rehab Robotics) feeding aid–based robot
B Wheelchair-mounted robots for training
2. First arm robot developed by Neville Hogan and his research group at Massachusetts Institute of Technology (MIT).86,87
3. The primary commercially available model for this is the Manus.
a. Currently manufactured by Exact Dynamics as iARM, ARM, and MIT-Manus.
b. Supports the shoulder and arm and assists movement of the arm.
c. Has a handpiece that can be used to help manipulate objects.
d. Upper-limb robot goes anywhere end-user takes the chair.
4. Raptor Rehabilitation Technologies, Division of the Applied Resources Corporation
5. Spitting Image (Jim Hennequin in United Kingdom)
6. Armeo (Hocoma) attached to chair and workstation (see virtual task practice)
7. WREX—Wilmington Robotic Exoskeleton (new model WREX II)
a. Can be attached to most common wheelchairs and seating systems (three different mounts and forearm support).
b. Exoskeleton approximates normal human anatomy.
c. Linear elastic bands are used for balance, provide antigravity lift, and assist movements.
d. Can be switched for right and left.
e. WREX II has a motor to assist the rubber bands to lift heavier things.
C Temporarily mounted but freely moving upper-limb robot: Jacob Rosen, University of California, Santa Cruz
D Freely moving wearable assistive upper-limb exoskeleton
1. MoVAR, Stanford University (the DeVAR on wheels)
2. KARES II robot system, developed at KAIST in Korea, with arm mounted on mobile base
3. Wessex robot (Bath Institute of Medical Engineering)
4. Myomo mPower 1000 for the elbow (see under biofeedback-assisted devices)
5. Armeo (see virtual practice)
6. Bioness L200 for the wrist (see under neuromuscular stimulation–assisted upper-limb robotics)
II. Wearable assistive robotic devices for task practice
A Virtual reality task practice
b. Used to perform virtual tasks at a workstation.
c. Supports affected arm and hand.
d. Facilitates self-initiated and intensive, repetitive movements within a three-dimensional environment.
e. Games are fun and provide feedback to facilitate motivation.
2. University of California, Santa Cruz upper-limb exoskeleton
a. Robot includes two arms; patients can train with one or both arms.
b. Exoskeleton has six degrees of freedom at the shoulder and four at the elbow and wrist.
c. Does not include a robotic hand.
d. Exoskeleton hooked to wall frame.
e. Patient performs virtual tasks.
f. Robot unweights the arm, decreases joint friction of the device, and on some games assists the patient in performance.
g. Robot measures kinematic data associated with the task performance.
h. Subject works in open space, but the exoskeleton is fixed to a support stand on the wall.
3. L-Exos system (University of Pisa, Italy)
a. Five degrees of freedom and force feedback.
b. Used to study the benefits of robotic-assisted virtual reality–based rehabilitation for chronic poststroke patients.
c. Patient sits with the right forearm (not left) in the exoskeleton.
d. Video projector displays a virtual scenario: a reaching task.
e. A motion task constrained to a circular trajectory and an object manipulation task are practiced.
f. Designed to be used in a fixed workspace.
g. On some tasks, the robot provides assistance; on other tasks, no guided assistance is provided, but the therapist can elect to unweight the arm.
h. Device is controlled by two concurrent impedance controls.
i. Reaching and following accuracy are calculated.
j. Patient cannot use the device to move around and perform a variety of daily activities.
1. Single task robots—The single-task robots carry out predefined tasks (e.g., eating) activated by simple input devices. The most successful example is the Handy 1.83
a. Manus Assistive Robotic Manipulator (iARM, ARM, MIT-Manus, Exact Dynamics)84
i. Wearable orthotic is activated and monitored based on myoelectric and visual signals.
ii. Robot is attached to the wheelchair; is available where the wheelchair is located.
iii. Patient puts on the exoskeleton and is able to use a gripper end-effector to perform tasks.
iv. Manus-HAND includes fingers with three joints.
v. Crossed tendon mechanism is used to control the amount of flexion and extension movements.
vi. Movement of the wrist is separate from movement of the hand.
vii. Dexterous nature of the hand is limited by the current actuation technology.
viii. Force sensors are present on the thumb and two fingers.
ix. There is real-time identification of electromyographic commands and computation of control loops and force biofeedback.99
x. Has a two-fingered gripper end-effector.
xi. Has six plus two degrees of freedom.
xii. User can control the Manus ARM by accessing menus on standard devices (e.g., keypad, joystick, or switch).
xiii. Patient can move each joint individually.
xiv. Vision system has two cameras mounted with the camera at the shoulder providing the perspective of the occupant and a camera within the gripper to provide a closer view of computer control.
xv. Task includes a gross reaching movement to the target and then fine motor control of the end effector to manipulate the object.
b. Mirror Image Mobilization Enabler (MIME) System (Department of Veterans Affairs Research and Development, Palo Alto, Calif).
ii. Uses an industrial available robot (PUMA) to apply forces to the paretic limb during three-dimensional movements to perform actual tasks
c. In Japan, two exoskeleton-based systems were developed at Saga University.
i. One-degree-of-freedom interface was designed for the elbow using a robot to interpret human subject intention.
ii. A newer two-degrees-of-freedom interface is used to assist human shoulder joint movement.
d. In Switzerland, the ARM was also developed with three degrees of freedom for shoulder and one degree of freedom for elbow actuation.
e. The Salford Exoskeleton is based on a pneumatic muscle actuator system (pMA) and provides power over weight ratios.
f. Gentle/S robotic assistance (Europe)—integrates haptic technologies with high-quality virtual environments to drive practice in patients with upper-limb impairments.85
III. Biofeedback and upper-limb robotic devices: actual task practice
A Myomo mPower 1000 exoskeleton for the elbow
1. It is a wearable assistive robotic device for facilitating control of the elbow.
2. It is programmed to sense patient effort (muscle firing) with elbow flexion and extension before providing assistance to the patient.
3. mPower 1000 is approved by the U.S. Food and Drug Administration (FDA) for use in the home or in the clinical setting.
4. Designed to pick up patient effort and then assist with elbow movement for patients after stroke, spinal cord injury, multiple sclerosis, cerebral palsy, muscular dystrophy, or traumatic brain injury.
5. Based on MIT-developed technology.
6. Fits like a sleeve on the arm.
7. Has sensors that are in contact with the skin and the muscles to detect even faint muscle signals.
8. When the person tries to move and the muscle fires, the robot will engage to assist in completing the desired movement.
9. Unit can be programmed to assist with elbow flexion, elbow extension, or both elbow flexion and extension.
10. Sensor electrodes are placed over the biceps and triceps.
11. Therapist selects the desired mode, and the patient practices object manipulation and task activities with assistance of one or both muscles.
12. Device is battery powered and allows the patient to move around when practicing.
13. The patient and the therapist create the tasks.
14. Robotic device does not include an end effector such as a hand or a claw.
B Hand Mentor (Kinetic Muscles)—another upper-extremity assistive robotic device that assists patients with repetitive practice of hand and wrist movements
1. Electrodes are applied to the forearm within a wearable exoskeleton to sense muscle contraction.
2. The patient is asked to participate in recruiting the muscles with some biofeedback regarding success.
3. With or without voluntary muscle contractions, the assistive device helps the patient move the wrist.
4. Device is used while the patient sits in a fixed place or position.
5. Functional task activities are not performed.
6. There is no end effector for the hand.
7. Patient focuses on extension or flexion of the wrist.
8. Unit must be plugged into the wall.
9. Designed primarily to train patients poststroke, but could be used for patients with other neurological diagnoses.
C AMES—assisted movement with enhanced sensation (upper limb)
1. Developed by Paul Cordo (Oregon).
2. Uses biofeedback regarding voluntary joint torque.
3. Sensation of motion enhanced by tendon vibration.
4. Initial trials with acute poststroke patients with severe impairments.
5. Effective at restoring functional movement in upper extremity in profoundly disabled acute poststroke patients.
6. Does not restore functional movement at fingers or wrist joints.
7. Product moving into the commercial market.
8. Some further development underway to try to convert electromyographic signals from voluntary muscle contractions into useful biofeedback on a graphic display.
IV. Neuromuscular stimulation and wearable upper-limb robotics to assist task practice
A Neuromuscular stimulation to facilitate upper-limb movements with assistive robotic devices
i. Surface electrodes on wrist muscles
ii. Assistive robotic device for stimulation of wrist flexors and extensors of the wrist
(a) Patient must have an intact peripheral nervous system.
(b) Operates on a battery, and the hand can be used as part of training.
(c) Muscles are stimulated, and the patient is instructed to move in the direction of the stimulation.
(d) One challenge is contractures of the finger flexors. When wrist extension is stimulated, the fingers go into flexion.
(e) Another challenge is excessive spasticity in the finger flexors making it difficult to open the hand even with stimulation of the extensors of the wrist and fingers.
2. Muscle-implanted electrodes for neuromuscular stimulation with assistive robotic devices (no commercial products in 2011).
3. Subdural implanted electrodes in brain to provide electrical stimulation to control limbs for patients after spinal cord injury. Current area of research in 2012 with promise for functional use in the clinic.
V. Brain-connected wearable upper-limb robotics
A Brain interfaces are being developed.
1. Control is by direct brain connections (surface electrodes).
2. When there are no other options to help patients control a limb or an exoskeleton using usual interfaces, the brain may become the primary connection.
1. Involve the control of a robot through a direct implantation of an electrode in the brain.
2. The patient only has to “think” about performing a task and the exoskeleton can move the limb with an end effector to perform the task.
3. Is the newest form of advanced technology and is currently directed toward the upper limb.
4. Research in this area is being completed at a variety of neuroscience and neurorehabilitation research laboratories.
5. Collaborations developing to use existing robotic devices and develop a brain interface.
6. Challenges regarding how long the electrode can remain in the brain (implanted in cortex or basal ganglia or embedded in subdural space).
BOX 38-13  GAIT TRAINING WEARABLE ASSISTIVE ROBOTIC DEVICES FOR THE LOWER LIMB
GAIT TRAINING WEARABLE ASSISTIVE ROBOTIC DEVICES FOR THE LOWER LIMB
I. Lower-extremity gait training wearable assistive robot
a. A wearable, unilateral, assistive robotic device, commercially available in 2009.
b. Exoskeleton is noninvasive: rigid and soft material.
c. Exoskeleton can fit right or left leg.
d. Uses sensors, a microprocessor, an actuator, and customized software to automatically detect a user’s action (e.g., walking or climbing stairs).
i. Actuator provides power assistance and resistance at knee.
ii. Sensory interface: responds to pressure (weight) in shoe insert to signal microprocessor to provide appropriate assistance:
(a) Extends knee when sensor is loaded.
(b) Releases knee extension when sensor is unloaded during heel off in swing phase of gait.
(c) Provides resistance (eccentric flexion) when sensor loaded and patient moving from standing to sitting or descending a stair.
iii. Combines a drive force system with an external support system.
e. Programmable to the individual patient in terms of:
ii. Amount of loading (threshold to activate) robotic device
iii. Amount of assistance in knee extension
iv. Amount of resistance (eccentric control of knee flexion)
g. Weighs approximately 5 pounds.
i. Helps with teaching patients to put weight on affected limb (especially those with neglect).
ii. Provides assistance with transitional movements.
iii. Enhances walking speed, endurance, and quality of gait.
iv. Seems to have carryover to assist ankle dorsiflexion.
v. Can also be used with an ankle-foot orthosis (AFO).
vi. Patients can practice walking indoors and outdoors independently.
B Bilateral robotic-assisted lower-extremity exoskeletons
a. Bilateral robotic exoskeleton for walking.
c. Device supports an upright posture and robotic-assisted walking.
d. Does not require a backpack or crutches.
e. Two large legs support and lift the user.
f. User controls the system with joysticks at his or her side on the exoskeletons.
g. Can be used by individuals who can self-transfer and operate hand controls.
h. Used mostly with patients with spinal cord injuries.
i. Suitable for patients with other orthopedic and neurological conditions.
j. Uses a rechargeable battery (runs for 2 hours; takes 3 to 4 hours to recharge).
k. Costs approximately $150,000 and is available only in New Zealand and England.
l. Programmable; provides assistance for both legs through sensors, microprocessors, and actuators controlled by a joystick.116
a. Initially referred to as eLEGS in Home Rehabilitation System; designed by Homayoon Kazerooni, University of California, Berkeley; manufactured by Berkeley Bionics)
b. Original step-in bilateral exoskeleton was used in war to assist a soldier to carry people and objects
c. Ekso Bionics (formerly Berkeley Bionics)
i. Integrates sensors in the crutches and the feet with computer-generated stepping of the legs, including flexion of the knee.
ii. Enables paraplegic patients to walk with a four-point gait.
iii. Model for gait training is being designed for patients poststroke.
iv. Patient has to have enough strength to rise from the chair or a wheelchair.
v. Easy to step into exoskeleton.
vi. Computer and battery carried in backpack.
vii. Primary advantages are that this exoskeleton:
(a) Can be used indoors and outdoors
(b) Allows individuals to take their first steps after five to ten sessions of training
(c) Can be worn over regular clothes
(d) Has a battery that lasts about 6 hours
(e) Allows users to attain a speed of 3 km/hr, which is close to the speed of a community ambulator
viii. Currently available to institutions for clinical use and for research.
ix. Scheduled to become commercially available for personal use and training in 2012.
a. Bilateral robotic exoskeleton.
b. Motorized gears move the legs.
c. Computer-equipped backpack with battery to power the device for 3 to 4 hours.
d. Motion sensors and onboard processing monitor the upper-body movements and center of gravity.
e. When user shifts the body, the device steps in the proper direction.
f. Patient uses stabilizing crutches.
g. Developed by Argo Medical Technologies.
h. Available for institutional training.
i. ReWalk for personal use will be available by the end of 2012.118
a. Cadence Biomedical walking system developed by Brian Glaister (Seattle, Washington) to assist with gait training in patients with weakness or loss of control of the lower limbs
b. Bilateral exoskeleton using springs to activate assistance at the hip and the ankle
d. Approved by the U.S. Food and Drug Administration for gait training.
e. Requires casting to fit the spring system into an exoskeleton.
5. STRING-MAN—wire robotic gait system
a. Integrates robotic technology with control algorithm.
b. Developed at Fraunhofer IPK, Berlin.42
c. Combines body-weight support with controlled weight suspension and postural control.
d. Provides automatic, comfortable, efficient, and adjustable preparation of the patient.
e. Has programmable system for controlling biomechanical patterns of gait.
f. Facilitates patient’s own initiatives and effort (assistive).
C Lower-limb assistive robotic devices with neuromuscular stimulation
i. Facilitates dorsiflexion and eversion through electrical stimulation.
ii. Activates firing via the peroneal nerve when tibia moves anteriorly just after roll off and through swing phase.
iii. Commercially available for rent or purchase.
iv. Programmable: amplitude, frequency, timing.
v. Unit includes electrodes in a cuff; can be worn on left or right.
i. Facilitates dorsiflexion and eversion through electrical stimulation.
ii. Activates firing via the peroneal nerve when heel lifted off ground at push off.
iii. Commercially available for rent or purchase.
iv. Programmable: amplitude, frequency, timing.
v. Unit includes electrodes in a cuff with controller around neck or in pocket.
vi. Can be worn on left or right, but best if patient has a left cuff and a right cuff.
vii. Has a walking mode and an exercise mode.
viii. Adjust amplitude to encourage joint effort of patient activation and electrical stimulation.
ix. With training, there has been improvement in dorsiflexion and eversion; sometimes device is no longer needed.
2. Implanted neuromuscular stimulation
a. Implant electrodes for single or multiple muscle groups.
b. For the ankle, implant electrodes for peroneal stimulation.
c. For sequential gait in patients with spinal cord injuries, implant a series of multiple electrodes for walking.
d. Facilitates sequential gait in patients with spinal cord injuries.
e. Eight- to 12-channel units have been implanted in several research studies for patients with partial cervical spinal cord injuries.
f. System has been well tolerated and reliable.
g. Has been associated with increased endurance and walking speed after 12 weeks of training.
h. Improves efficiency with practice.
i. Advantages: decreases skin irritation, can decrease amplitude necessary for activation.
j. Disadvantages: needles may be uncomfortable; can get infected.
k. Expensive and not necessarily user friendly for patient to use alone.
D Biofeedback-facilitated assistive robotic devices
1. Foot Mentor (Kinetic Muscles)
a. Uses the same Mentor Pro device as the Hand Mentor.
b. Has different programs to facilitate foot dorsiflexion and extension exercises.
c. Picks up biofeedback cues from patient when asked to engage the muscles.
d. Assists the patient into the desired movements.
2. AMES—assisted ankle movement with enhanced sensation
a. Uses biofeedback of voluntary joint torque.
b. Sensation of motion enhanced by tendon vibration.
c. Effective at restoring functional movement in lower extremity in profoundly disabled chronic stroke patients.
d. Did not restore functional movement at the ankle joint.
e. Continued development to try to convert electromyographic signals into useful biofeedback on a graphic display.











In 2012, there were a variety of wearable upper-limb robotic devices on the market, and most were unilateral (see Box 38-12). At the same time, there were fewer lower-limb wearable robotic devices on the market; however, a variety of lower-limb exoskeletons are under development10,11,35,94 (see Box 38-13).
Effectiveness of wearable assistive robotic devices.
The effectiveness of wearable assistive robotic devices is promising. Assistive robotic devices for the lower limb have been positively associated with short- and long-term gains in gait speed, quality of gait, endurance, time in single leg stance, toe clearance, and balance.35,115,119,120 There is also positive evidence supporting the effectiveness of training with a neuroprosthetic ankle-foot gait trainer, with short- and long-term gains reported in gait speed, endurance, safety, and quality.122–126
For upper-limb assistive robotic training, there are positive trends for improving motor control, particularly in patients poststroke.84,96,105,106,127–143 Unfortunately, based on a systematic review of upper-limb robotics,132,133 improved function in task performance and object manipulation was not necessarily correlated with improved motor control. The gains in motor control appear to be greatest when one-on-one care is supplemented with robotic training.
Research studies also report improved motor control with the integration of a neuroprostheses in functional arm training (e.g., includes neuromuscular stimulation or biofeedback).82,144–146 However, although there are greater gains in motor control, these gains are not necessarily associated with improved function.146
Emotional interactive entertainment and friendly robots.
Emotional interactive entertainment robots (EIARs) are similar to VR systems. EIAR systems are designed for communication and emotional support.147 EIAR devices can increase emotional comfort and give emotional relief to people who live alone.
Entertainment robots are mechatronic devices that exhibit animal-like behaviors.
For example, within the project Home Information Infrastructure House (HII) house, National Panasonic introduced a user-friendly home interface for older people as a memory jogger (e.g., cuddly toys). The speech synthesis can reproduce phrases and can be programmed to remind users to take their medications at a particular time. Failure to respond can activate a direct call to a caregiving staff member who can then check on the user. BECKY,148 a friendly robot from Korea, demonstrates different behaviors according to the emotional status of the user. The seal robot and the cat robots from Japan149,150 provide interactions between hospitalized human patients and the pet robots. The Autonomous Robotic Remedial Activity (AuRoRA) Project151,152 applied robots to education and therapy for children with autism.
Screening patients for the integration of robotic technology
General screening
An objective evaluation is needed to match a patient with a commercially available robotic device. This evaluation must include a thorough assessment of anatomical, physiological, cognitive, and sensory impairments. Whenever possible, standardized tests should be used to document strength, flexibility, endurance, balance, coordination, synergistic responses, hypertonicity, gait, balance, posture, and postural righting skills. These impairments need to be integrated into functional and task-specific assessments of motor learning, motor control, activities of daily living (ADLs), work requirements, and recreational needs. Then each patient should be screened by defined objectives relative to outcomes in terms of quality of life and independence. Subjective and emotional issues such as attention, motivation, history of positive health behaviors, durability, depression, desire for independence, and commitment to learning must also be considered. Many of these assessment tools are described in Chapter 8. The challenge is to determine if achieving rehabilitation goals requires integration of advanced technology and whether the patient has the potential to be trained to benefit from the prescribed technology.
Specific screening by type of robotic device
Table 38-2 summarizes some screening criteria that could be used by the therapist to determine if a patient can include rehabilitation technology into the plan of care in order to maximize function. This table also summarizes the level of function required by the patient to be able to effectively use robotic technology to improve independence and quality of life. The criteria to assess patient needs and abilities are classified by type of robotic technology. The criteria are neither all-inclusive nor exclusive but serve as a starting point for a therapist to make a recommendation for this type of technology to be considered.
TABLE 38-2 
| ASSISTIVE ROBOTIC DEVICES | |||
| SCREENING CRITERIA | SERVICE ROBOTIC DEVICES | NONWEARABLE—MOBILITY AND UNWEIGHTING | WEARABLE—MOBILITY AND OBJECT MANIPULATION |
| Criteria for determining potential benefit for patient to integrate advanced or robotic technology | Patient with severe physical impairments challenged to be independent without personal assistance:
1. Has significant weakness of trunk and limbs (0, trace, poor) 2. Has minimal voluntary control of trunk and limbs 3. Cannot use a manual chair independently 4. Requires personal assistance to transfer to and from chair 5. Cannot step without maximum assistance 6. Unable to walk or stand independently |
1. Has impaired ability to walk
2. Has poor or slow balance responses
3. Demonstrates unstable single-limb support (unilateral or bilateral)
5. Could benefit from fall protection when standing
6. Is weak (has poor strength)
7. Has difficulty initiating stepping
8. Lacks high-quality voluntary control for walking
9. Has involuntary synergistic movements
11. Uses an assistive mobility device
12. Needs to reduce ground reaction forces when walking or during intense exercise owing to pain, inflammation, osteoporosis, joint replacement, incoordination, and so on
13. Walks very slowly (household ambulatory but limited community ambulation)
14. Must maintain cardiopulmonary and metabolic health
15. Could benefit from stimulation of neurotransmitters and endorphins
1. Is unable to perform common daily tasks for independence without an assistive device or personal assistance
2. Needs assistance at one or more joints
3. Needs assistance to complete a task
4. Takes excessive time to complete task
5. Needs assistive device to ensure stability to walk
6. Has experienced a fall or an injury when performing a daily task (e.g., toileting)
7. Cannot live safely alone without personal assistance
8. Cannot cross the street in time
9. Needs more controlled forced task practice
10. Needs assistance to improve quality
11. Is not afraid of computerized or electromechanical devices
12. Is learning “abnormal” movements
13. Lives alone, but safety is in question
14. Drives but needs some assistance with transfers and/or arm or leg movements
1. Has cognitive ability to control motorized and robotic devices
2. Has the sensory, physical, and cognitive abilities to control a motorized chair (e.g., via joystick, head movement, button press, breath, piezoelectricity, voice) without human assistance
3. Can activate an automated harness system to transfer into a wheelchair
4. Can sit in a chair with or without positional assistance
5. Has sufficient understanding and ability to activate robotic service and emergency devices to be independent without human assistance (smart house designs)
1. Has cognitive ability to participate in training
2. Has sufficient attention and understanding to cooperate in gait training
3. Has adequate head and trunk control to maintain postural uprightness when legs moving
4. Has sufficient strength in legs to stand up when unloaded or protected from falling
5. Has some sensation in lower limbs or can see legs
6. Has partial movement in major muscle groups in lower limb (hip, knee, ankle)
7. Has sufficient range of motion to get into standing or walking position
8. Can transfer onto the treadmill or transfer from chair to standing
9. Tone does not prevent the feet from staying on the ground or stepping when unloaded
10. Has ability to step when standing over ground or over treadmill
11. Steps after perturbation of the treadmill
12. Can swing leg through clearing floor or treadmill (with or without AFO).
1. Has intellectual ability to understand how to use the wearable assistive orthotic device
2. Has the ability to don the wearable assistive device (or has someone at home to help)
3. Is motivated to use a wearable assistive robotic device to improve independence
4. Has basic stability of the head and trunk to move the limb(s) (even if positioning device is required)
5. Involuntary movements do not interfere with robotic assistance
6. Has adequate standing balance (with or without cane or walker) to work with a wearable assistive orthotic gait training exoskeleton
7. Has the range of motion to allow full or partial task function
8. Has adequate sensation to sense rubbing and chaffing of orthotic device
9. If inadequate sensation, has sufficient vision, audition, touch, or cognition to monitor wear and control of interface
10. Has adequate strength to lift the weight of the exoskeleton
11. Has sufficient voluntary control to assist the exoskeleton
12. Able to use the robotic assistive device several hours per day
13. Has the physical, sensory, sensorimotor, and/or cognitive skills to control the interface of the assistive robotic device
14. If unable to meet 13, may be eligible for advanced technology using a brain interface
1. Goals and objectives to be functionally independent without personal assistance
2. Predictable disease- or impairment-specific issues that are not going to change or may get worse
3. A support system (family or community) to check on status at home
4. Home that can be modified to accommodate robotic equipment
1. Goals and objectives to be functionally independent without personal assistance
2. Predictable disease- or impairment-specific issues that necessitate regular exercise to maintain independence
3. A progressive neurodegenerative condition that could be slowed with regular exercise
4. A support system (family or community) to check on status at home
5. Access to public transportation to access resources
6. The ability to drive (e.g., take driver’s training or simulation; car modification) to maintain independent access to needed resources
1. Goals and objectives to be functionally independent without personal assistance
2. Predictable disease- or impairment-specific issues that require regular exercise to maintain and maximize independence despite injury or disease
3. Ability to maintain if not maximize independence despite injury
4. Ability to use robotic technology to improve functional recovery
5. Ability to put on and remove the assistive devices
6. Ability to slow down progression or maintain or improve function despite neurodegenerative condition that could be slowed with protected, guarded, stress-reduced intense exercise
7. A support system (family or community) to check on status at home
8. Access to public transportation to achieve community independence
9. Ability to maintain independent community driving with regular training, simulation, car modification
1. Safely step on and off the treadmill
2. Tolerate the tension of the harness or unweighting system
3. Spontaneously step as triggered by the moving treadmill
4. Express concern if exercising beyond his or her limits
5. Manipulate the parameters of the treadmill
6. Tolerate the end range parameters for performance (e.g., high speed)
1. Adequate sensation to notice increased pressure or chaffing or skin sensitivity to electrodes
2. Ability to decrease the hypertonicity that interferes with function or causes pain
3. Sufficient cognitive awareness to recognize abnormal robotic behaviors (e.g., forced movement in abnormal directions)
4. Ability to stop excessive, abnormal movements
5. Ability to initiate self-directed movements with robotic assistance
1. Access to financial resources to afford advanced technology
2. Access to technology that is currently commercially available
3. Access to technology that is currently accessible in his or her geographical area
4. Opportunity to arrange for technical help to maintain equipment
1. Objective outcomes as measured by decreased personal assistance, which can be documented in terms of hourly costs saved
2. That resource investment costs can be amortized across 5 years
3. That patients could gain 5-10 years of independent function at home
4. That the patient would be able to sustain independence at home (versus in skilled living environment) in the last few months of life
1. Objective outcomes focused on maintaining independence at home in lieu of an extended care facility
2. Patient can minimize falls and decrease risks for inpatient stay resulting from fall injuries
3. Patient able to sustain safe, independent indoor navigation without personal assistance
4. Patient able to get out of house and move in community independently or with public transportation
1. Objective outcomes focused on maintaining independence at home
2. Patient can perform ADLs and community activities safely
3. Patient uses assistive devices to minimize risk of falls
4. Patient remains committed to brain and physical fitness
5. Patient maintains safe, independent indoor and outdoor navigation without personal assistance
6. Patient able to get out of house and move in community independently or with public transportation
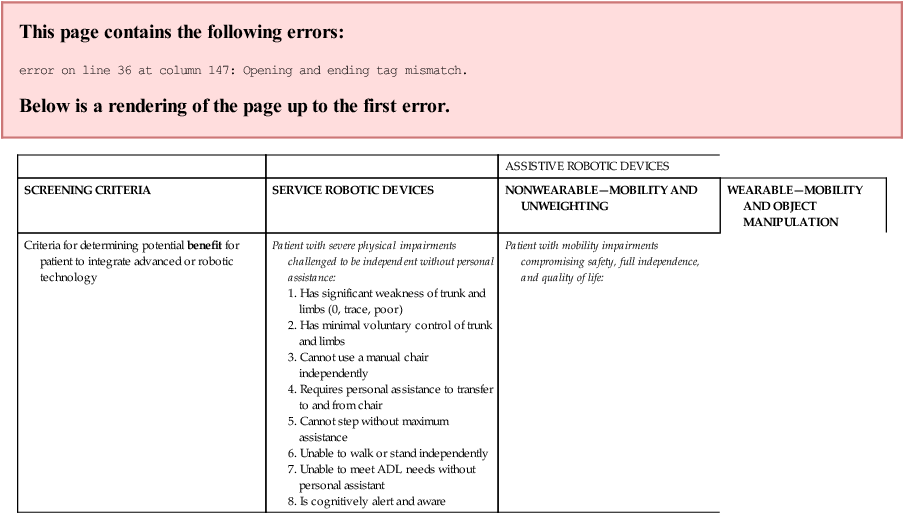
Specific screening of patients for assistive nonwearable robotic technology: example of body-weight–supported gait training technology systems
The patient needs to go through general and specific screenings to determine the appropriateness of integrating a nonwearable assistive robotic device into the rehabilitation program (see Table 38-2). The patient who is most likely to benefit from body-weight–supported gait training is the patient who has the prognosis for functional independence but needs to train to improve quality, endurance, speed, and stability of gait. Thus many patients with problems described within this text might benefit from this type of training. Those who do not have the potential for independent ambulation could still benefit from training on a BWSTS. In these cases, the training would be directed toward enhancing metabolic health, providing a sense of well-being, increasing circulation, and minimizing secondary impairments associated with excessive sitting such as decubitus ulcers and bone demineralization. These patients may need robotic, human, or harness assistance to achieve standing or stepping as well as bracing of the neck and trunk when upright. Patients with joint pain in the back or knee may also benefit from wearing supports when standing or exercising.
In spite of advancements in rehabilitation robotic technology, some patients may still have difficulty taking advantage of this type of therapeutic assistance (Box 38-14). In patients with challenging impairments, for safety the use of an overhead harness to access the treadmill may be required, in addition to close supervision by one or more therapists.
BOX 38-14  MATCHING PATIENTS TO EFFECTIVE WEARABLE ROBOTIC DEVICES
MATCHING PATIENTS TO EFFECTIVE WEARABLE ROBOTIC DEVICES
1. How much force can the robot safely exert to overcome resistance from hypertonicity?
2. How strong does the patient need to be to overcome the weight of the wearable assistive robotic device?
3. Does the robot need to be programmed across multiple joints to move with high-quality movements?
4. Does the robot need to stop if the individual does not initiate movement in the exact pattern of the programmed assistance?
5. Is there negative learning when there is a mismatch between the patient’s movements and the robotic assistance?
6. Can the amount of assistance provided be dynamically controlled by the robot while being based on the patient’s need for task performance?
7. Can the therapist or the patient easily modify the assistance given by the wearable robotic device?
Specific screening of patients for wearable assistive devices
Most patients with temporary or permanent sensory, motor, or structural impairments can benefit from training with a dynamic wearable assistive device. However, there are currently no guidelines that can be applied to assist a clinician with objective screening. Some screening criteria have been developed to try and match patients to devices, with a focus on safety.10,11,86,94,153–157
Screening must be sensitive to the characteristics of the individual and consistent with factors in Table 38-2. After identifying the parameters of performance and the potential benefits of assistive wearable technology, the patient, the family, the therapist, and sometimes the orthotist should determine what assistive robotic devices or advanced technological equipment are available to meet the patient’s needs. The team also has to assess where the devices are located, whether they are accessible, whether the device should be rented or purchased, and whether the insurance company will help pay for the rental or purchase of the device.
In addition to the general and specific screening criteria, it is important to note that some assistive robotic devices may target control of one specific joint. However, given the biomechanical links, flexibility and sensory and motor characteristics must be assessed at each major joint above and below the primary assisted joint. For example, the Tibion Bionic Leg (see Figure 38-8, A) focuses on assisting the knee, but the patient’s hip and ankle also should be assessed. The less affected side also needs to be evaluated. To maximize the benefit of a wearable assistive device, patients should ideally have some ability to voluntarily initiate movement and a grade of poor or greater strength to be able to assist in the movement.
Wearable robotics must be programmed to assist patient function but also to stop to avoid harm. This requires a balance between the dynamic nature of the wearable assistive device and a patient’s weakness, lack of voluntary motor control, and the presence of involuntary muscle activity including hypertonicity (e.g., spasticity, dystonia, rigidity, tremor) (Box 38-14). For example, how much force would the assistive device need to provide to overcome involuntary tone? Other relevant questions must then be asked: If a robotic device is programmed to assist with flexion and the patient initiates movement into extension or abduction, will the robot have to stop assisting the limb to prevent harm? If the robot stops assisting, is there a negative effect caused by the mismatch of force between the patient and the robot? Does the patient need consistent assistance or variable assistance? How will the therapist, the robot, or the patient determine how much assistance is needed? In one case a patient may need unweighting of only a limb, and in another case both unweighting and assistance may be needed. In theory, the amount of assistance needed should decrease with recovery of function. Thus it is helpful if the wearable assistive device can easily be adjusted by the therapist or the patient.
Despite the advancements in rehabilitation robotics, some patients will still have difficulty wearing an assistive orthotic. For example, wearable assistive orthotic devices may not work well for patients with severe sensory impairments, severe balance problems, a fear of falling, or inadequate assets to control the device or for elderly patients who are afraid of computerized technology (see Box 38-15). Sophisticated rehabilitation robotic devices may also not be recommended for patients who are disoriented, who have severe pain or neural hypersensitivity, or who cannot don the apparatus independently (Box 38-16).
BOX 38-15  IMPAIRMENTS THAT INTERFERE WITH UNWEIGHTED GAIT TRAINING
IMPAIRMENTS THAT INTERFERE WITH UNWEIGHTED GAIT TRAINING

Related posts:
 Differential diagnosis phase 1: medical screening by the therapist
Differential diagnosis phase 1: medical screening by the therapist
 Balance and vestibular dysfunction
Balance and vestibular dysfunction
