[level-membership-for-dermatology-category]
Infestations
Infestation is defined as the harbouring of insect or worm parasites in or on the body. Worms – on or in the skin – are infrequent except in tropical countries. Insect life on the skin is usually transient in temperate climes, although a mite (Demodex folliculorum) may live harmlessly in facial hair follicles.
Insects cause a variety of skin reactions (Table 1). Contact with an insect or an insect bite can produce a chemical effect, such as a bee sting, or an irritant effect, such as dermatitis from contact with a caterpillar or blistering due to cantharadin released from a crushed beetle. Contact may also cause an immune-mediated response.
Table 1 Insect effects on the skin
| Insect | Effect |
|---|---|
| Animal ticks | Bites, disease vector |
| Ants, bedbugs, fleas | Bites |
| Bees, wasps | Stings |
| Caterpillars | Dermatitis |
| Cheyletiella | Papular urticaria |
| Demodex folliculorum | Normal inhabitant |
| Food and harvest mites | Bites |
| Lice | Infestation (bites), disease vector |
| Mosquitoes | Bites, myiasis, disease vector |
| Sarcoptes scabei | Scabies |
Insects act as vectors of skin disease, as in Lyme disease (p. 51), when animal ticks transmit Borrelia burgdorferi. They involve the skin directly by burrowing (e.g. scabies) or by laying eggs that hatch into larvae (myiasis).
Insect bites
Clinical presentation
The lesions of insect bites vary from itchy wheals (Fig. 1) through papules to quite large bullae (Fig. 2). The morphology will depend on the insect (Table 1) and the type of response elicited. Insect bites are usually grouped or track up a limb. Papular urticaria defines recurrent itchy urticated papules on the limbs or trunk, quite often in a child. The culprits, which may be difficult to trace, include garden insects, fleas or mites on household pets. Bedbugs cause bites on the face, neck and hands. They lie inactive in crevices in furniture during the day and emerge at night. Secondary bacterial infection of excoriated insect bites is common.


Lice infestation (pediculosis)
Lice are flat, wingless, blood-sucking insects (Fig. 3). Their eggs (nits) are laid on hairs or clothing. There are two anthropophilic species:
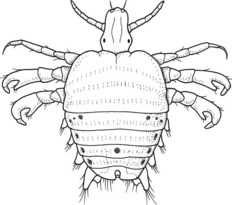
Head lice are common among schoolchildren and spread by head-to-head contact. The nits are often easier to see than the lice (p. 20). The body louse is mainly seen in vagrants who live in unhygienic or poor social conditions. Spread is by infested bedding or clothing. The pubic louse is sexually transmitted and is mostly found in young adults. Lice induce intense itching which, through scratching, results in excoriation and secondary infection.
Clinical presentation
The itching of head lice usually starts at the sides and back of the scalp. Scratching results in secondary infection that may cause matted hair. Body lice result in excoriations on the trunk and, in chronic infestation, lichenification and pigmentation. The lice are found in the seams of clothes. Pubic lice, known colloquially as ‘crabs’, result in severe pruritus with secondary eczema and infection. They may involve the eyelashes. Lice infestation should not be confused with other conditions (Table 2).
| Louse infestation | Differential diagnosis |
|---|---|
| Body louse | Scabies, chronic eczema |
| Head louse | Impetigo, eczema |
| Pubic louse | Scabies, eczema |
Management
Head lice are treated with malathion or phenothrin lotion, applied to the scalp for 12 h, washed out and repeated in 7 days. Dimeticone is an alternative. Nits are removed by wet combing. Contacts are also treated. Body lice are eradicated by treating the clothing with tumble drying, laundering or dry cleaning. Malathion or permethrin lotions may be used on the skin. Infestation with pubic lice requires the application of malathion or permethrin aqueous lotions to all the body. Sexual partners should be treated.
Scabies
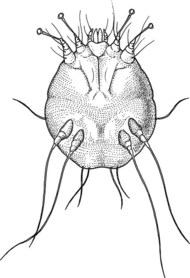
The scabies mite, Sarcoptes scabei var. hominis, is 0.4 mm in length (Fig. 4) and is spread by direct physical transfer, including sexual contact. The fertilized female mite burrows through the stratum corneum at the rate of 2 mm/day, laying two or three eggs each day. The eggs hatch after 3 days into larvae, which form shallow pockets in the stratum corneum where they moult and mature within about 2 weeks. The mites mate in the pockets; the male dies, but the fertilized female burrows and continues the cycle. After first being infested, it takes 3–4 weeks for the hypersensitivity reaction to the mite, and the intense itching that it causes, to develop. On average, about 12 mites are present at the itching stage, but it can be many more.
Clinical presentation
The irregular, tortuous and slightly scaly burrows measure up to 1 cm long. They are commonest on the sides of fingers (Fig. 5), wrists, ankles and nipples, and on the genitalia where they form rubbery nodules. Small vesicles are often seen. Itching induces excoriations (Fig. 6). In infants, the feet are frequently involved and the face can be affected. The mite is occasionally visible as a white dot at the end of a burrow. If extracted with a needle and viewed under a microscope, the diagnosis is irrefutable.


Complications
Scabies commonly becomes secondarily infected. In institutionalized or immunosuppressed patients, very large numbers of mites proliferate to produce an extensive crusted eruption known as ‘Norwegian’ scabies (p. 118).
Management
 Apply the lotion or cream to the entire body surface including scalp, face, neck and ears.
Apply the lotion or cream to the entire body surface including scalp, face, neck and ears.
 Pay special attention to fingerweb and toeweb spaces, and under the nails.
Pay special attention to fingerweb and toeweb spaces, and under the nails.
 Leave the lotion on for 12–24 h and then wash off in the bath or shower.
Leave the lotion on for 12–24 h and then wash off in the bath or shower.
 If the hands are washed during this period, reapply the lotion or cream.
If the hands are washed during this period, reapply the lotion or cream.







[/level-membership-for-dermatology-category][not-level-membership-for-dermatology-category]
Infestations
Infestation is defined as the harbouring of insect or worm parasites in or on the body. Worms – on or in the skin – are infrequent except in tropical countries. Insect life on the skin is usually transient in temperate climes, although a mite (Demodex folliculorum) may live harmlessly in facial hair follicles.
Insects cause a variety of skin reactions (Table 1). Contact with an insect or an insect bite can produce a chemical effect, such as a bee sting, or an irritant effect, such as dermatitis from contact with a caterpillar or blistering due to cantharadin released from a crushed beetle. Contact may also cause an immune-mediated response.
Table 1 Insect effects on the skin
| Insect | Effect |
|---|---|
| Animal ticks | Bites, disease vector |
| Ants, bedbugs, fleas | Bites |
| Bees, wasps | Stings |
| Caterpillars | Dermatitis |
| Cheyletiella | Papular urticaria |
| Demodex folliculorum | Normal inhabitant |
| Food and harvest mites | Bites |
| Lice | Infestation (bites), disease vector |
| Mosquitoes | Bites, myiasis, disease vector |
| Sarcoptes scabei | Scabies |
Insects act as vectors of skin disease, as in Lyme disease (p. 51), when animal ticks transmit Borrelia burgdorferi. They involve the skin directly by burrowing (e.g. scabies) or by laying eggs that hatch into larvae (myiasis).
Insect bites
Clinical presentation
The lesions of insect bites vary from itchy wheals (Fig. 1) through papules to quite large bullae (Fig. 2). The morphology will depend on the insect (Table 1) and the type of response elicited. Insect bites are usually grouped or track up a limb. Papular urticaria defines recurrent itchy urticated papules on the limbs or trunk, quite often in a child. The culprits, which may be difficult to trace, include garden insects, fleas or mites on household pets. Bedbugs cause bites on the face, neck and hands. They lie inactive in crevices in furniture during the day and emerge at night. Secondary bacterial infection of excoriated insect bites is common.
Lice infestation (pediculosis)
Lice are flat, wingless, blood-sucking insects (Fig. 3). Their eggs (nits) are laid on hairs or clothing. There are two anthropophilic species:
[/not-level-membership-for-dermatology-category]
