[level-membership-for-obstetrics-gynecology-category]
Chapter 38 Induction of labour
Assessing the cervix
The cervix remains closed because of its rigidity due to the collagen fibres that make up the bulk of cervical stroma. Cervical connective tissue consists mainly of collagen and a matrix of large proteoglycan molecules.
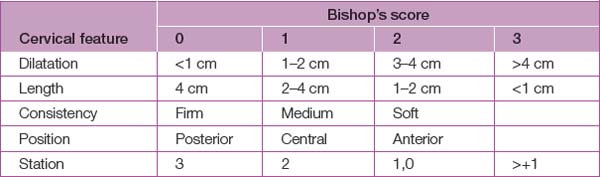
A uniform means of assessing the cervix is the Bishop’s score (see Table 38.1). The Bishop’s score assesses the favourability of the cervix for induction of labour by assigning points to each of the five cervical features and adding these points. With a low score (0–3), there is a high risk of a failed induction, resulting in caesarean section (>20%), compared with a score of 8 or more, where the failed induction rate is <3%. With a high score, the cervix is said to be ‘ripe’.
Induction of labour
Indications
Contraindications
Table 38.2 lists contraindications for induction of labour.
| Absolute | Relative |
|---|---|
| Absolute cephalopelvic disproportion | Antepartum haemorrhage |
| Presumed fetal distress | Grand multiparity |
| Placenta praevia | Previous caesarean section |
| Vasa praevia | Overdistended uterus |
| Abnormal presentation | Face or breech presentation |
| Previous classical caesarean section | History of rapid labour |
| Invasive carcinoma of cervix | |
| Cord presentation |
Techniques of induction
Surgical
Medical
Oxytocin
Augmentation of labour
Bishop E.H. Pelvic scoring for elective induction. Obstetrics and Gynecology. 1964;24:266.
Grant J.M. Sweeping the membranes in prolonged pregnancy. British Journal of Obstetrics and Gynaecology. 1993;100:889-890.
Hannah M., Hannah W.J., Hellmann J., et al. Induction of labor as compared with serial antenatal monitoring in post-term pregnancy: a randomized controlled trial. Canadian Multicenter Post-Term Pregnancy Trial Group. New England Journal of Medicine. 1992;326(24):1587-1592.
[/level-membership-for-obstetrics-gynecology-category][not-level-membership-for-obstetrics-gynecology-category]
Chapter 38 Induction of labour
Assessing the cervix
The cervix remains closed because of its rigidity due to the collagen fibres that make up the bulk of cervical stroma. Cervical connective tissue consists mainly of collagen and a matrix of large proteoglycan molecules.
A uniform means of assessing the cervix is the Bishop’s score (see Table 38.1). The Bishop’s score assesses the favourability of the cervix for induction of labour by assigning points to each of the five cervical features and adding these points. With a low score (0–3), there is a high risk of a failed induction, resulting in caesarean section (>20%), compared with a score of 8 or more, where the failed induction rate is <3%. With a high score, the cervix is said to be ‘ripe’.
