[level-membership-for-radiology-category]

 . Abrupt, short segment narrowing is typical of malignant lesions.
. Abrupt, short segment narrowing is typical of malignant lesions.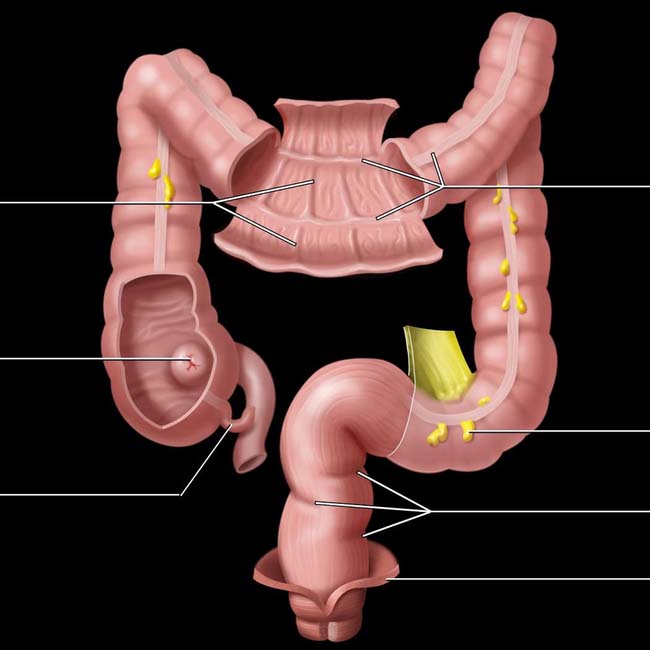
Ileocecal valve
Appendix
Taeniae coli
Epiploic appendage
Rectal valves
Levator ani muscle
(Top) Graphic shows the surface and mucosal views of the colon. Three flat bands of smooth muscle, the taeniae coli, run the length of the colon. The semilunar folds lie at right angles to the taenia creating the haustra.
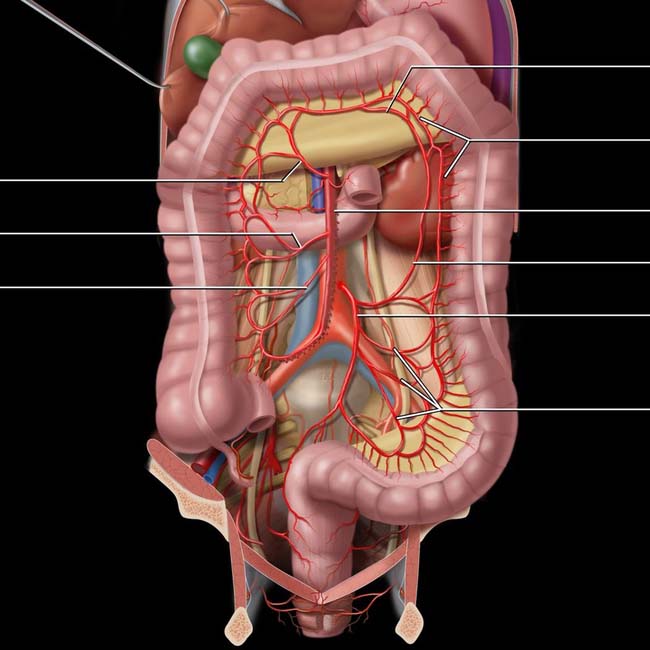
Right colic artery
Ileocolic artery
Arc of Riolan
Marginal artery (of Drummond)
Superior mesenteric artery
Left colic artery
Inferior mesenteric artery
Sigmoid arteries
(Bottom) The superior mesenteric artery supplies the colon from the appendix through the splenic flexure, with the inferior mesenteric artery supplying the descending colon through the rectum. These arterial branches are highly variable. All are connected by anastomotic arterial arcades and by the marginal artery (of Drummond) and arc of Riolan, which also anastomose with branches of the inferior mesenteric artery that feed the descending and sigmoid colon.
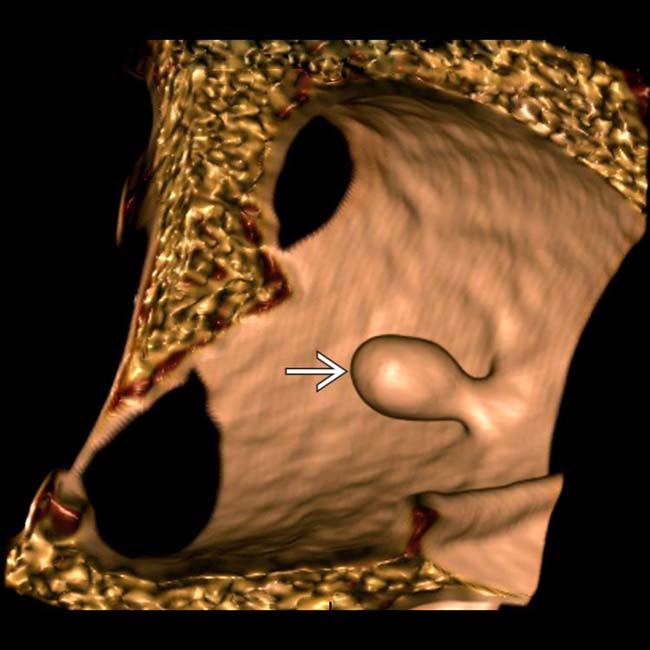
 . This 6 mm lesion was subsequently removed via conventional colonoscopy and found to be a benign adenomatous polyp.
. This 6 mm lesion was subsequently removed via conventional colonoscopy and found to be a benign adenomatous polyp.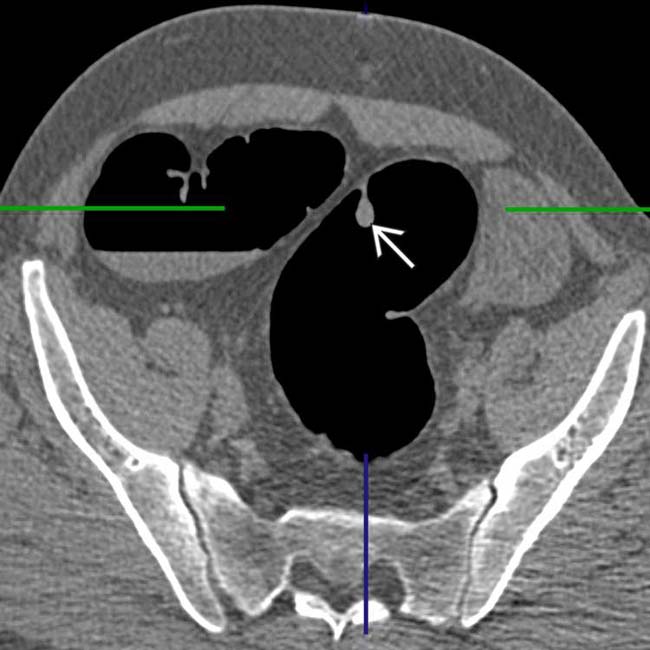
 outlined by the insufflated carbon dioxide.
outlined by the insufflated carbon dioxide.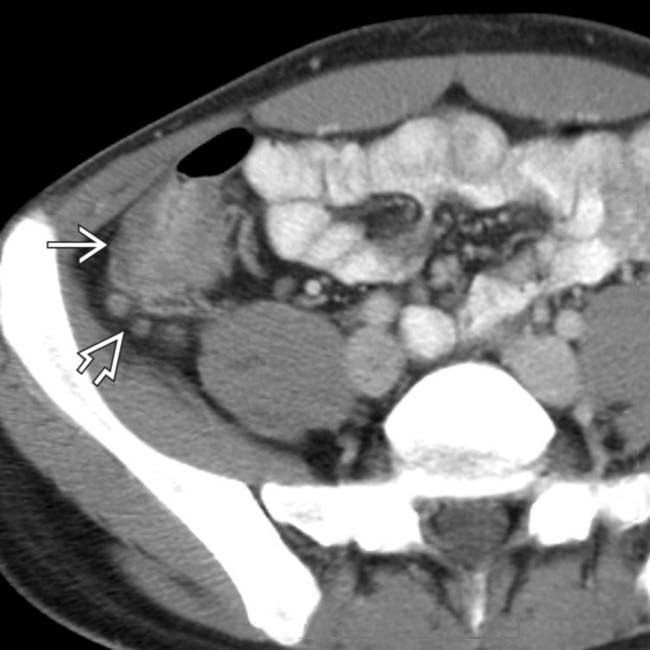
 , with infiltration of the mesentery and enlarged regional nodes
, with infiltration of the mesentery and enlarged regional nodes  .
.
 . These are typical features of Crohn disease, confirmed in this case, but infectious enteritis may have a similar appearance.
. These are typical features of Crohn disease, confirmed in this case, but infectious enteritis may have a similar appearance.
 , and a circumferential soft tissue density mass
, and a circumferential soft tissue density mass  in the cecum with extensive invasion into adjacent tissues.
in the cecum with extensive invasion into adjacent tissues.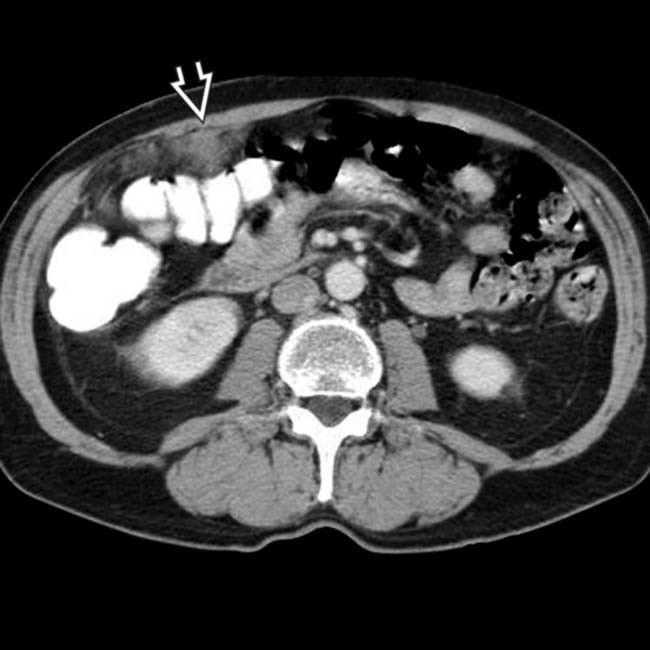
 , essentially diagnostic of metastatic malignancy. At surgery, this and the cecal carcinoma were confirmed and resected.
, essentially diagnostic of metastatic malignancy. At surgery, this and the cecal carcinoma were confirmed and resected.
 of the sigmoid colon and ascites
of the sigmoid colon and ascites  . The rectum
. The rectum  was normal. These are classic clinical and CT features of ischemic (hypoperfusion) colitis.
was normal. These are classic clinical and CT features of ischemic (hypoperfusion) colitis.
 affecting the entire colon, including the rectum. These are classic clinical and imaging features of infectious colitis. Enteropathic Escherichia coli (0157: H7 subtype) was the etiology.
affecting the entire colon, including the rectum. These are classic clinical and imaging features of infectious colitis. Enteropathic Escherichia coli (0157: H7 subtype) was the etiology.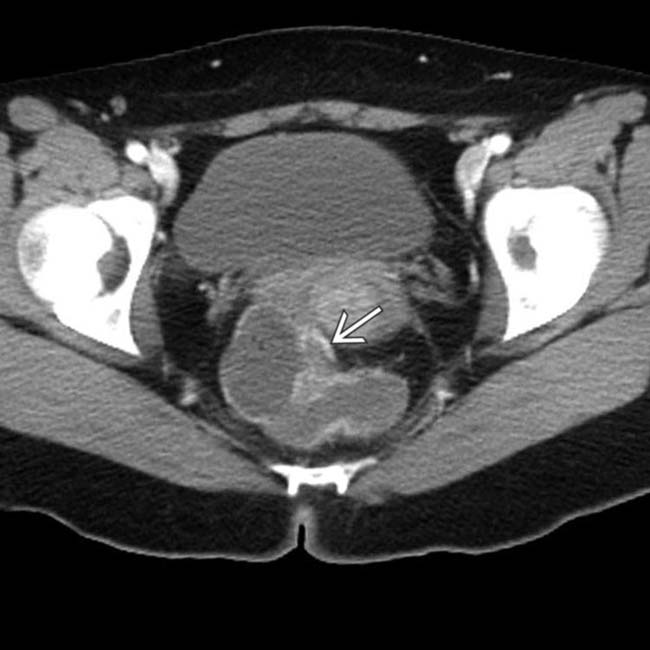
 . The rectum is rarely involved in ischemic colitis.
. The rectum is rarely involved in ischemic colitis.
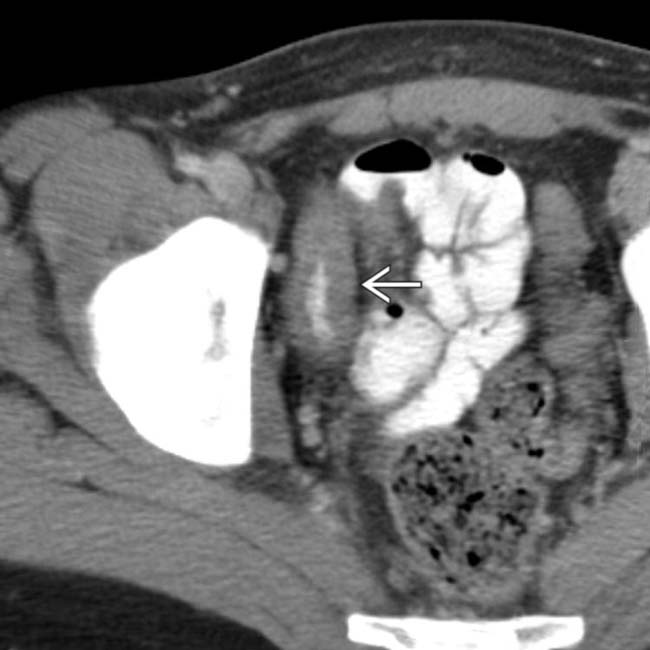
 , the vagina
, the vagina  , and a colovaginal fistulous tract
, and a colovaginal fistulous tract  . The cause was diverticulitis, infecting a hysterectomy scar.
. The cause was diverticulitis, infecting a hysterectomy scar.
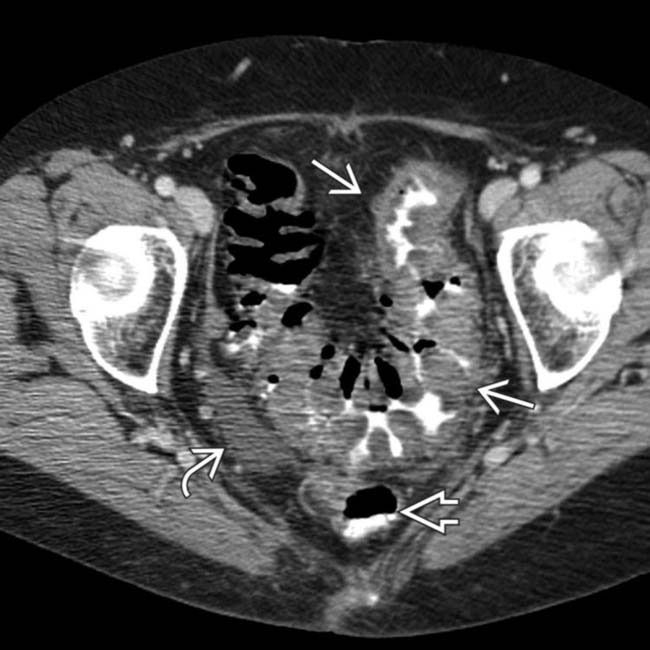
 to the vaginal cuff with contrast filling the vaginal lumen
to the vaginal cuff with contrast filling the vaginal lumen  .
.[/level-membership-for-radiology-category][not-level-membership-for-radiology-category]
. Abrupt, short segment narrowing is typical of malignant lesions.Ileocecal valve
Appendix
Taeniae coli
Epiploic appendage
Rectal valves
Levator ani muscle
(Top) Graphic shows the surface and mucosal views of the colon. Three flat bands of smooth muscle, the taeniae coli, run the length of the colon. The semilunar folds lie at right angles to the taenia creating the haustra.
Right colic artery
Ileocolic artery
Arc of Riolan
Marginal artery (of Drummond)
Superior mesenteric artery
Left colic artery
Inferior mesenteric artery
Sigmoid arteries
(Bottom) The superior mesenteric artery supplies the colon from the appendix through the splenic flexure, with the inferior mesenteric artery supplying the descending colon through the rectum. These arterial branches are highly variable. All are connected by anastomotic arterial arcades and by the marginal artery (of Drummond) and arc of Riolan, which also anastomose with branches of the inferior mesenteric artery that feed the descending and sigmoid colon.
[/not-level-membership-for-radiology-category]
