[level-membership-for-radiology-category] arising from the superior mesenteric artery. The left gastric artery also has a separate origin from the aorta, though difficult to perceive on this image. The “celiac trunk” in this patient consists only of the splenic artery. Congenital variations of vascular anatomy are very common.
arising from the superior mesenteric artery. The left gastric artery also has a separate origin from the aorta, though difficult to perceive on this image. The “celiac trunk” in this patient consists only of the splenic artery. Congenital variations of vascular anatomy are very common.

 from the superior mesenteric artery.
from the superior mesenteric artery.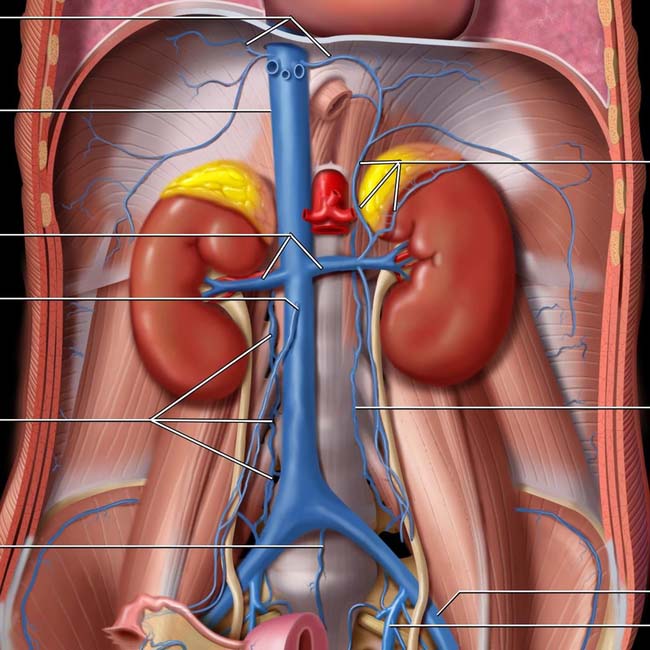
Inferior vena cava (IVC)
Renal veins
Right gonadal vein
Ascending lumbar vein
Middle sacral vein
Adrenal veins
Ascending lumbar vein
External iliac vein
Internal iliac (hypogastric) vein
(Top) The inferior vena cava (IVC) is formed by the confluence of the common iliac veins, which are formed by the confluence of the internal and external iliac veins. Note the ascending lumbar veins, which anastomose freely between the IVC and azygous, hemiazygos, and renal veins. These form a pathway for collateral flow in the event of IVC obstruction and play an important role in the systemic spread of pelvic tumors and infection.
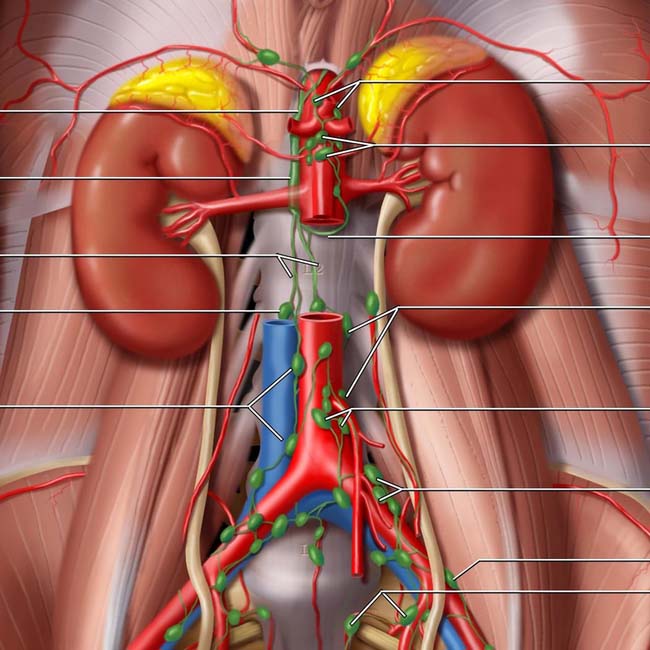
Cisterna chyli
Lumbar trunks (of cisterna chyli)
Right lumbar (retrocaval) node
Aortocaval nodes
Celiac nodes
Superior mesenteric nodes
Intestinal trunk (of cisterna chyli)
Lumbar (paraaortic) nodes
Inferior mesenteric nodes
Common iliac nodes
External iliac node
Internal iliac (hypogastric) nodes
(Bottom) The major lymphatics and lymph nodes of the abdomen are located along, and share the same name as, the major blood vessels.

 and retrocrural
and retrocrural  lymph nodes.
lymph nodes.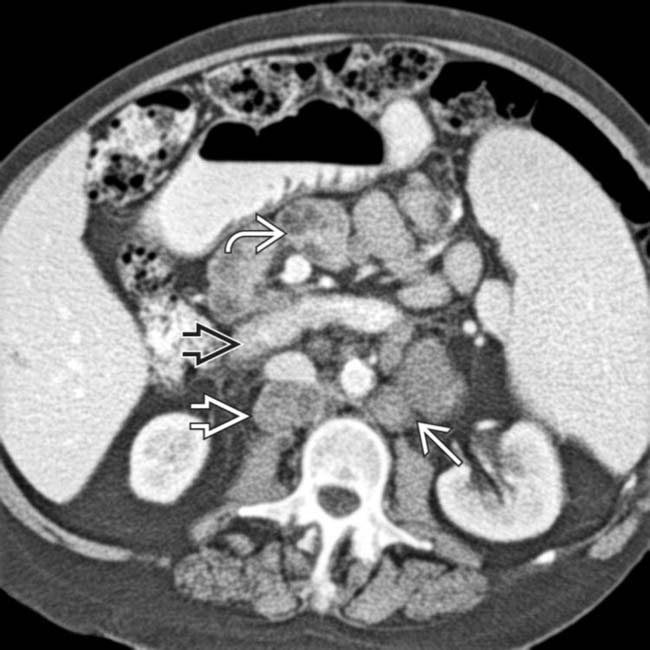
 is displaced by large retroperitoneal nodes; the mesenteric vessels are surrounded or “sandwiched” by mesenteric nodes
is displaced by large retroperitoneal nodes; the mesenteric vessels are surrounded or “sandwiched” by mesenteric nodes  . The lumbar nodes are often referred to as para- or retroaortic
. The lumbar nodes are often referred to as para- or retroaortic  (or -caval)
(or -caval)  , indicating their position relative to the great vessels.
, indicating their position relative to the great vessels.
 .
.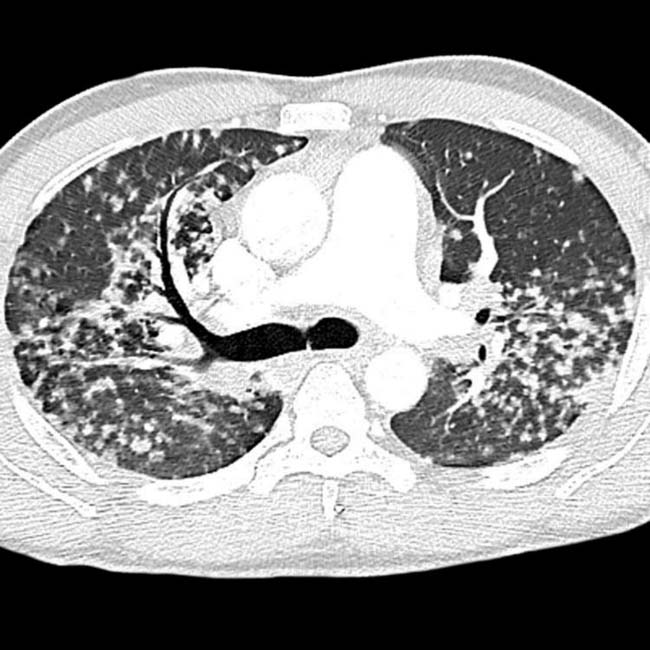

 in both kidneys, as well as upper abdominal lymphadenopathy
in both kidneys, as well as upper abdominal lymphadenopathy  .
.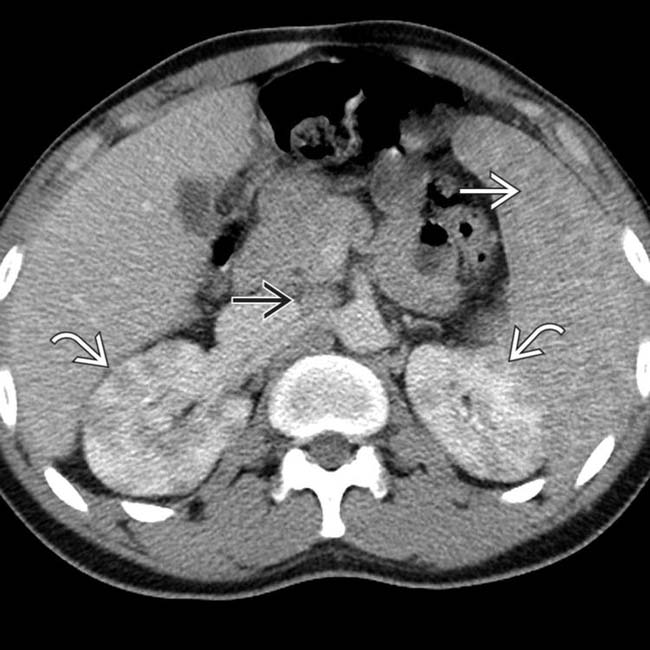
 , renal
, renal  , and nodal
, and nodal  disease. All lesions were found to represent sarcoidosis and responded to steroid medication.
disease. All lesions were found to represent sarcoidosis and responded to steroid medication.
 .
.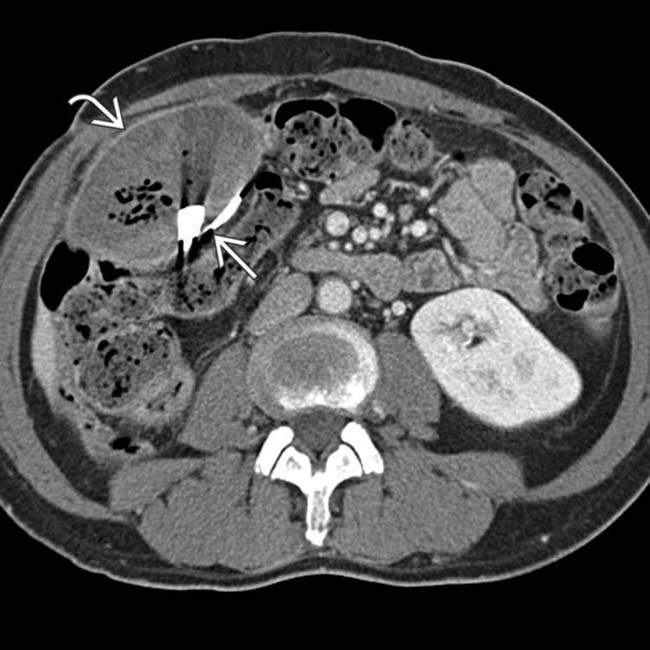
 with an adjacent thin, radiopaque structure
with an adjacent thin, radiopaque structure  that corresponds to the stripe seen on the radiograph. This is a classic gossypiboma, a retained surgical sponge that has resulted in a chronic abscess or foreign body reaction.
that corresponds to the stripe seen on the radiograph. This is a classic gossypiboma, a retained surgical sponge that has resulted in a chronic abscess or foreign body reaction.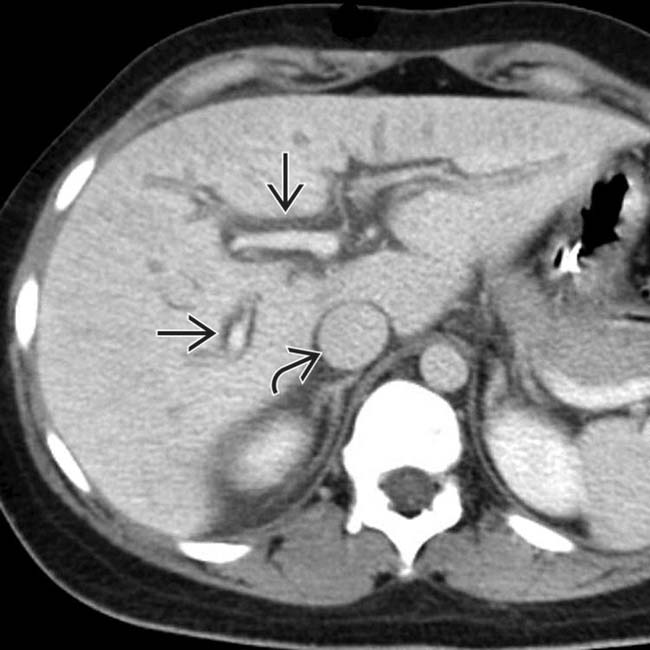
 and periportal edema
and periportal edema  , which might be mistaken for dilated bile ducts or hepatic injury.
, which might be mistaken for dilated bile ducts or hepatic injury.
 in the Morison pouch. There was no hemoperitoneum nor visceral injury. The findings were due to aggressive IV hydration of the patient and resolved by the following morning.
in the Morison pouch. There was no hemoperitoneum nor visceral injury. The findings were due to aggressive IV hydration of the patient and resolved by the following morning.
 .
.
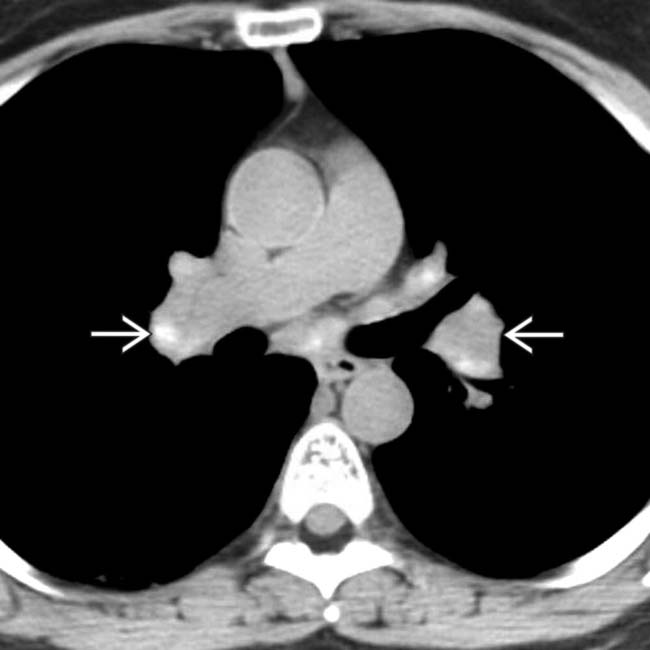
 including some calcification.
including some calcification.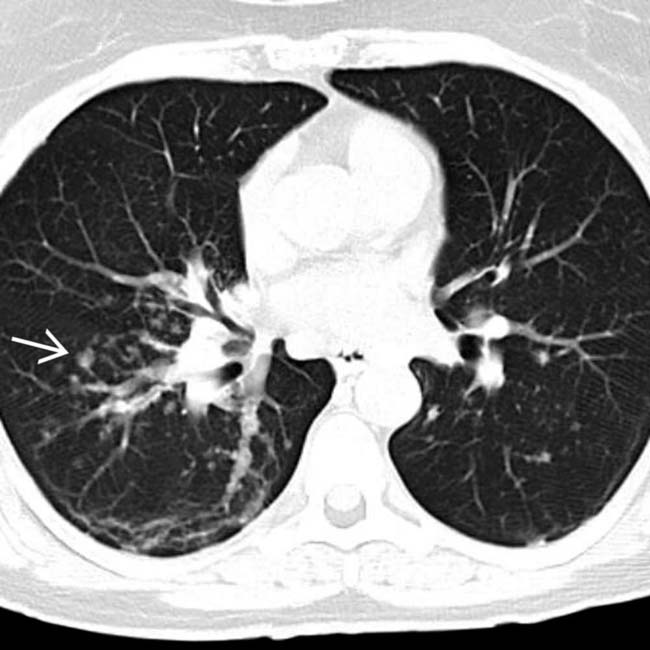
 , characteristic of pulmonary sarcoid.
, characteristic of pulmonary sarcoid.
 is a clue to the presence of sarcoid in these organs.
is a clue to the presence of sarcoid in these organs.
 , as another manifestation of sarcoidosis.
, as another manifestation of sarcoidosis.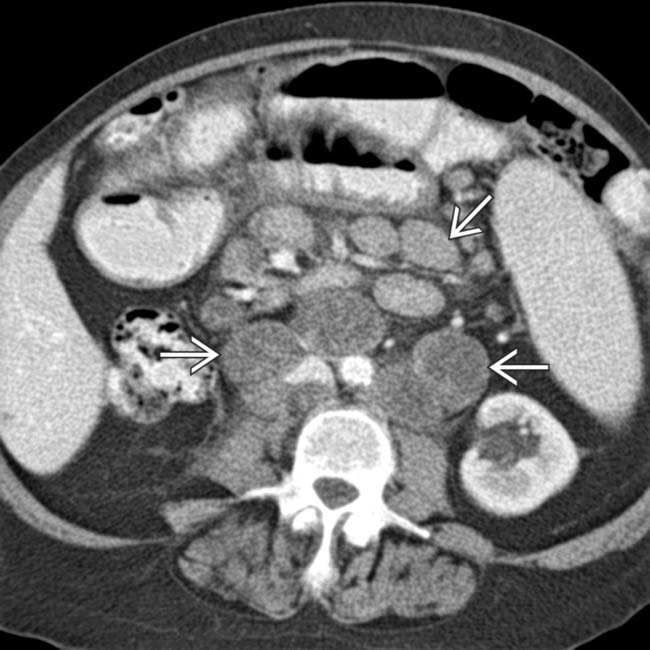
 that are massively enlarged and of unusually low attenuation, all due to NHL.
that are massively enlarged and of unusually low attenuation, all due to NHL.
 follow the major blood vessels and have similar names, such as these external iliac nodes.
follow the major blood vessels and have similar names, such as these external iliac nodes.
 .
.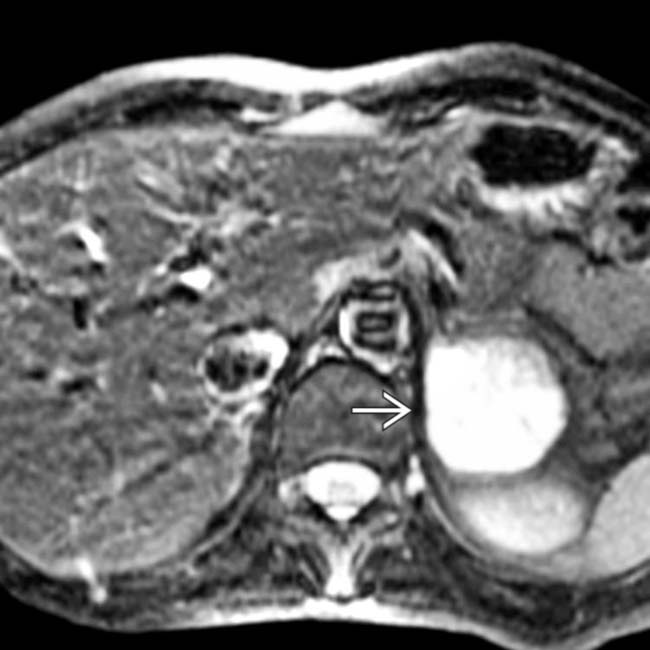
 that is heterogeneously hyperintense. This pheochromocytoma was not symptomatic but was detected in screening this patient with a medullary thyroid cancer, who was felt to be at risk for multiple endocrine neoplasia (MEN) syndrome.
that is heterogeneously hyperintense. This pheochromocytoma was not symptomatic but was detected in screening this patient with a medullary thyroid cancer, who was felt to be at risk for multiple endocrine neoplasia (MEN) syndrome.
 consistent with a renal cell carcinoma. Patients with von Hippel-Lindau are at risk for multiple and recurrent tumors of the kidneys and CNS. Imaging is critical to detect these at a potentially curable stage.
consistent with a renal cell carcinoma. Patients with von Hippel-Lindau are at risk for multiple and recurrent tumors of the kidneys and CNS. Imaging is critical to detect these at a potentially curable stage.
 and 1 of many cysts
and 1 of many cysts  in the kidneys.
in the kidneys.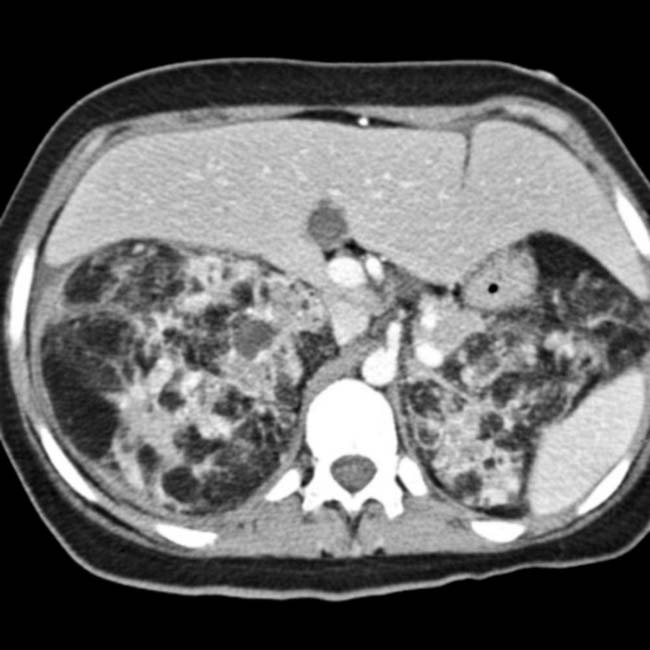

 that are characteristic of tuberous sclerosis complex.
that are characteristic of tuberous sclerosis complex.
 that are typical of plexiform neurofibromas of the lumbosacral plexus.
that are typical of plexiform neurofibromas of the lumbosacral plexus.
 that proved to be a ganglioneuroma.
that proved to be a ganglioneuroma.[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] arising from the superior mesenteric artery. The left gastric artery also has a separate origin from the aorta, though difficult to perceive on this image. The “celiac trunk” in this patient consists only of the splenic artery. Congenital variations of vascular anatomy are very common.
from the superior mesenteric artery.Inferior vena cava (IVC)
Renal veins
Right gonadal vein
Ascending lumbar vein
Middle sacral vein
Adrenal veins
Ascending lumbar vein
External iliac vein
Internal iliac (hypogastric) vein
(Top) The inferior vena cava (IVC) is formed by the confluence of the common iliac veins, which are formed by the confluence of the internal and external iliac veins. Note the ascending lumbar veins, which anastomose freely between the IVC and azygous, hemiazygos, and renal veins. These form a pathway for collateral flow in the event of IVC obstruction and play an important role in the systemic spread of pelvic tumors and infection.
Cisterna chyli
Lumbar trunks (of cisterna chyli)
Right lumbar (retrocaval) node
Aortocaval nodes
Celiac nodes
Superior mesenteric nodes
Intestinal trunk (of cisterna chyli)
Lumbar (paraaortic) nodes
Inferior mesenteric nodes
Common iliac nodes
External iliac node
Internal iliac (hypogastric) nodes
(Bottom) The major lymphatics and lymph nodes of the abdomen are located along, and share the same name as, the major blood vessels.
and retrocrural lymph nodes. is displaced by large retroperitoneal nodes; the mesenteric vessels are surrounded or “sandwiched” by mesenteric nodes . The lumbar nodes are often referred to as para- or retroaortic (or -caval) , indicating their position relative to the great vessels..[/not-level-membership-for-radiology-category]
