Chapter 14 Ilioinguinal, Iliohypogastric, and Genitofemoral Nerves and Lateral Cutaneous Nerve of the Thigh
Sensory Distributions of the Nerves
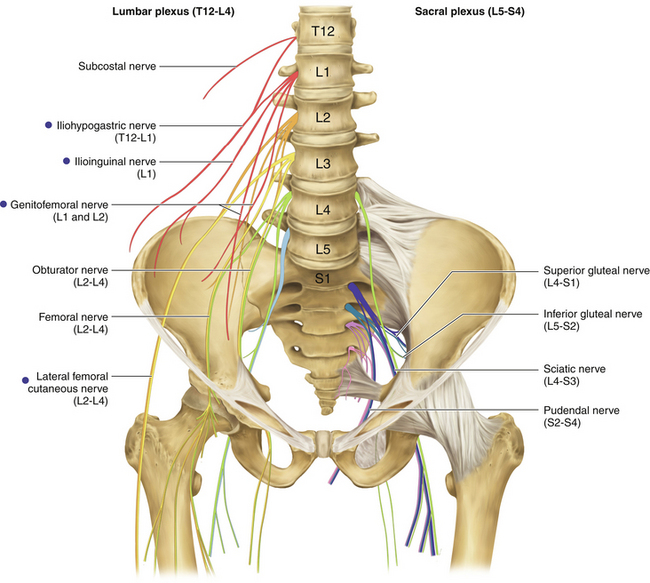
• These nerves originate from lumbar spinal nerves (Figure 14-1).
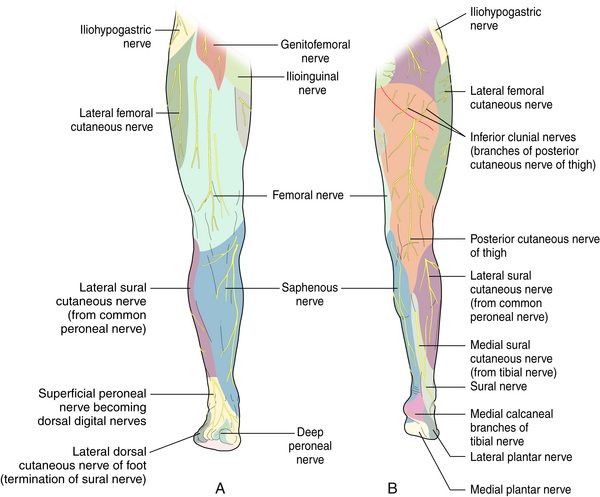
• The distribution of sensory changes and the nature of symptoms associated with injuries to these nerves overlap; however, with experience, they can usually be differentiated (Figure 14-2).
• The lateral femoral cutaneous nerve (LFCN) (L2 and L3) supplies the “trouser pocket” area (the anterolateral proximal thigh).
• The ilioinguinal nerve (L1) runs along the spermatic cord in males and the round ligament of the uterus in females. supplies sensation to the region of the symphysis pubis and medial thigh and, in males, to the dorsum of the penis and some of the upper scrotum. In females, the mons pubis and labia majora receive sensory input.
• The iliohypogastric nerve (L1) supplies some sensation to the lower abdominal skin above the pubis and also gives a lateral branch to the superior gluteal area.
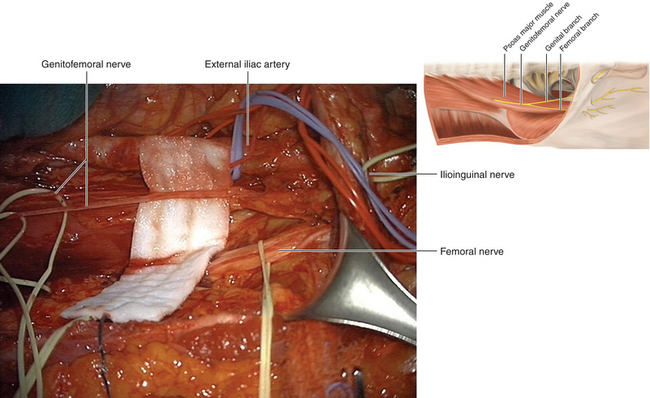
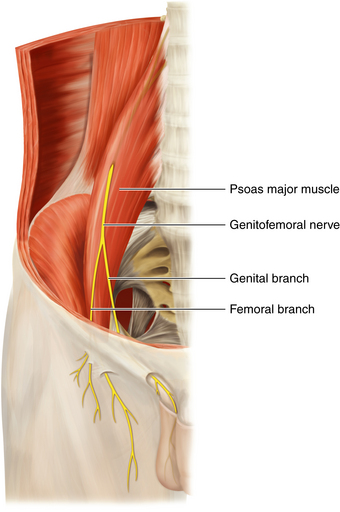
• The genitofemoral nerve (L1 and L2) divides into a genital branch, which innervates the cremaster muscle and scrotal skin in males and the round ligament in females, and a femoral branch, which innervates the skin in the region of the femoral triangle (Figure 14-3).
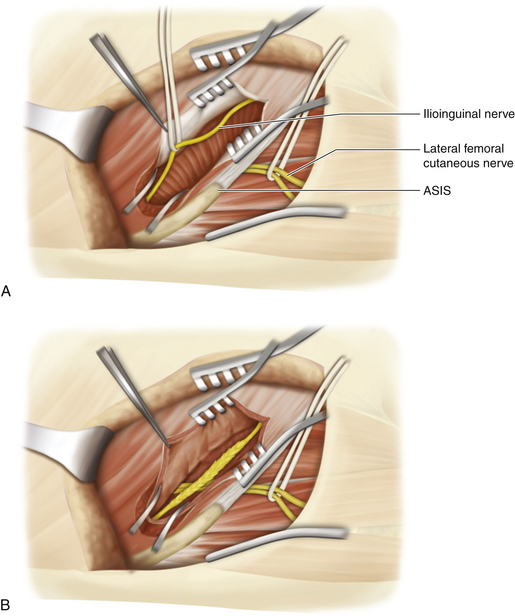
• The LFCN runs across the posterior abdominal wall, across the iliacus behind the iliac fascia, then through that fascia until it enters the thigh behind the inguinal ligament. The relationship of the nerve to the anterior superior iliac spine (ASIS) is variable; it usually lies within 1 inch medial to ASIS but occasionally runs just above the spine or, rarely, through it. Occasionally, the LFCN fascicles will stick to the femoral nerve and enter the thigh more medially than usual. Branches of the nerve pierce the fascia that invests the thigh at variable points, usually about 2 inches distal to the ligament.
• The ilioinguinal nerve runs laterally and down across the posterior abdominal wall to about the level of the iliac crest, where it enters the body wall. The iliohypogastric nerve runs a parallel course, at a higher level. The genitofemoral nerve runs downward on the anterior surface of the psoas major.
Surgical Technique
Lateral Femoral Cutaneous Nerve of Thigh
• The real key to operating on the LFCN is simply to find it. A less-experienced surgeon may try (without success) to find the nerve in the subcutaneous fat close to the ASIS and just distal to the inguinal ligament. However, the nerve is not encountered there, as it lies deep to the deep fascia at this point.
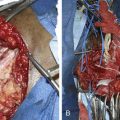
• A vertical or horizontal incision is made over the course of the nerve, and the fascia is exposed (Figure 14-4). The fascia is opened and a branch of the LFCN is identified. That branch is followed proximally to the main nerve within its fibrous tunnel, immediately below the ligament (Figure 14-5).
• As in any operation on an entrapment, the object is to decompress the entrapment point. In this case, there are two entrapment points: one within the fibrous tunnel and one more proximal within the fibrous fascia of the iliacus. The nerve is decompressed at the ligament by releasing the fibrous tissue. The operator then slides a finger up and over the nerve for 1 inch, to ensure that the second entrapment point is also lysed.
• An alternative is a small muscle split just above and medial to the ASIS. The nerve is found in the extraperitoneal space, proximal to its passage through or under the inguinal ligament.
• In complex repeat operations, the nerve is cut at this extraperitoneal site.

Ilioinguinal Nerve
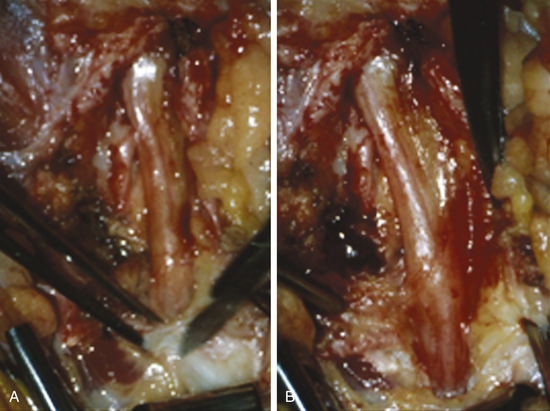
• Operatively, the ilioinguinal nerve is usually found beneath the external oblique muscle, proximal to the injury site, except at the flank level, where it is found between the internal oblique and transversalis muscles (Figure 14-6).
• The incision is placed above the ilium for exposure of the ilioinguinal or iliohypogastric nerve. A similar incision to that used for a lower abdominal quadrant muscle-splitting exposure of the distal pelvic portion of the femoral nerve can be used.
• Usually, the prior incision is extended laterally. Then the external oblique muscle is split lateral to the site of previous surgery (Figure 14-7).
• Normal nerve is identified laterally as it penetrates the internal oblique to run medially beneath the external oblique.
• If a lesion such as a neuroma is found, the injured nerve is resected.
• Often, scar tissue from previous procedures makes precise dissection difficult. In such cases, the nerve is identified on the posterior abdominal wall and is sectioned there.
• Genitofemoral branches penetrate the rectus abdominis and can be hard to find. The area of the scar is resected, along with the injured nerve and its branches (see Figure 14-4). In complex repeat surgery, the nerve is isolated well proximal to the injury site and is severed in the retroperitoneal space (Figure 14-8).
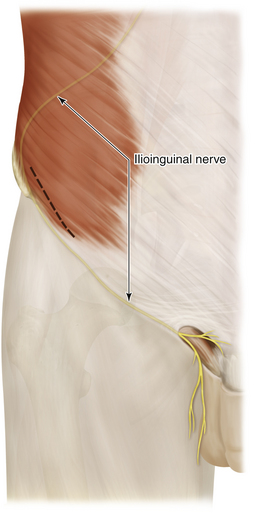
Figure 14-6 The course of the ilioinguinal nerve through the body wall to the external inguinal ring.