Tip of feeding tube should be located beyond stomach (distal duodenum or jejunum)
• Nasogastric tubes
Large-bore, moderately stiff
Used for temporary bowel decompression
Tip placed in pylorus can cause outlet obstruction
• Gastrostomy and jejunostomy tubes
Balloon-tipped catheters should not be placed into small bowel (may obstruct lumen)
Small amount of free air after placement is common and usually does not require intervention
IMAGING
• Malposition is most frequent complication of feeding tubes
Can be visualized on chest or abdominal radiograph
Auscultation over abdomen is not reliable method for confirming proper tube placement
CLINICAL ISSUES
• 1-3% of feeding tubes enter tracheobronchial tree
Anywhere from trachea to pleural space
Can perforate lung with significant morbidity and mortality
• Tube may penetrate esophagus or duodenum with fatal results
Often through diverticula (e.g., Zenker), due to thin wall
• High-risk patients
Altered mental status
Absent gag reflex
Multiple or repetitive insertion attempts
• Treatment
Reposition feeding tube if in incorrect location
Perforation of lung or bowel may require surgery
(Left) Esophagram shows a retroesophageal collection of gas and contrast medium resulting from perforation of a Zenker diverticulum by attempted placement of a feeding tube whose track runs parallel to the proximal esophagus.
(Right) Chest radiograph shows a feeding tube that has entered the right bronchus and perforated the lung though a lower lobe bronchus. The tip lies in the pleural space, a procedural complication that may be fatal, especially if food is given through the tube.
(Left) Frontal radiograph shows the peculiar course of the feeding tube with abrupt upper deviation of its distal portion. CT showed that the tube had perforated the duodenum and had been advanced with its wire in place.
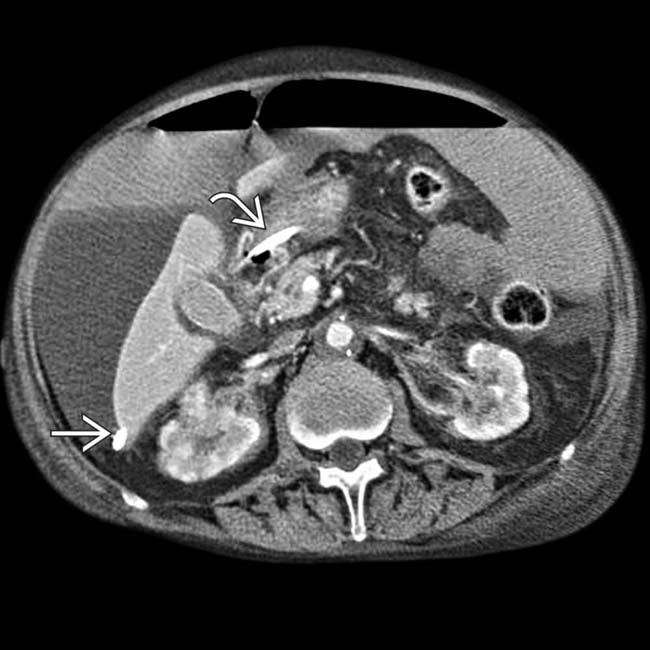
(Right) Axial CECT shows a feeding gastrostomy tube entering the stomach. The balloon tip of the tube has migrated into the jejunum where it is partially occluding its lumen.
TERMINOLOGY
Definitions
• Patient injury caused by improper feeding tube placement
• Feeding tubes
Small, soft enteric tubes
Some with flexible metallic tips
Used for feeding chronically ill patients
Can be used for long periods of time
• Nasogastric tubes
Large-bore, moderately stiff
Used for temporary bowel decompression or fluid sampling
Tip placed in pylorus can cause gastric outlet obstruction
• Gastrostomy and jejunostomy tubes
Placed surgically, endoscopically, or percutaneously
Used for long-term, possibly permanent, feeding
Use imaging to visualize tube balloon, surgical clips, and cuff
– Cuff initiates soft tissue reaction to anchor tube to abdominal wall
PEG button can replace tube several weeks post placement
– Placed in anterior abdominal wall
Balloon-tipped catheters should not be placed into small bowel
– Likely to obstruct bowel lumen
IMAGING
General Features
• Best diagnostic clue
Malposition is most frequent complication of feeding tubes
– Check on chest or abdominal radiograph
Usual course: Nares/mouth → esophagus → stomach → small bowel
• Location
Tip of feeding tube should be located beyond stomach
– In distal duodenum or proximal jejunum
Imaging Recommendations
• Best imaging tool
Chest or abdominal radiograph
Radiography is most accurate way to detect malposition/complications
– Obtain chest film after initial placement, followed by abdominal film
Electromagnetically guided placement systems are also in use
Auscultation over abdomen is not reliable method for detecting proper tube placement
Radiographic Findings
• Inadvertent placement in airways
Metal tip or stiffening wire can perforate lung
Administration of formula → empyema
• Malposition in esophagus
Can enter stomach and then coil back into esophagus
• Aspiration of gastrointestinal contents
Secondary to malposition in esophagus, pharynx, or stomach
Clue: Bilateral pulmonary infiltrates
• Perforation of gastrointestinal tract
Can perforate esophagus (e.g., Zenker diverticulum) or duodenum
• Gastrointestinal hemorrhage
May irritate and ulcerate mucosa
• Knotted tubing
Due to coiling, often within stomach
Can result in tube malfunction due to obstruction
• Complications of PEG tubes
Free intraperitoneal air
– Usually does not require intervention
Injury to abdominal structures (liver, colon)
Gastrointestinal obstruction
– Secondary to migration of balloon tip into pylorus or duodenum
– Do not put Foley catheter through PEG tube track
CLINICAL ISSUES
Presentation
• Most common signs/symptoms
• Other signs/symptoms
Respiratory distress
– Cough, dyspnea, cyanosis
– Not always present
Aberrant pH of aspirate
– Limited by use of proton-pump inhibitors
Demographics
• Epidemiology
1-3% of feeding tubes lodge in airways
• High-risk patients
Altered mental status
Absent gag reflex
Multiple or repetitive insertion attempts
Treatment
• Reposition feeding tube if in incorrect location
DIAGNOSTIC CHECKLIST
Consider
• Radiographic confirmation is best way to ascertain proper tube position
• Feeding tubes can move spontaneously
Position should be confirmed on each radiograph
In the same patient, the long extraluminal portion of the feeding tube is evident.
In the same patient, the point of perforation of the tube through the lateral wall of the duodenum is noted .
In the same patient, the point of perforation of the feeding tube through the lateral wall of the duodenum is noted .
CT in the same patient shows the feeding tube free in the peritoneal cavity. Placement of tube feedings through this tube resulted in free intraperitoneal gas and complex fluid.
CT shows that a long portion of a feeding tube is free in the peritoneal cavity.
In the same patient, supine radiography shows both the inside and outside of the bowel wall , a well-recognized (Rigler) sign of pneumoperitoneum.
Supine radiography shows massive free intraperitoneal gas, which outlines the peritoneal cavity . Both the inside and outside of the bowel wall are seen , a well-recognized (Rigler) sign of pneumoperitoneum. The external portion of the PEG tube is seen .
Tip of feeding tube should be located beyond stomach (distal duodenum or jejunum)
• Nasogastric tubes
Large-bore, moderately stiff
Used for temporary bowel decompression
Tip placed in pylorus can cause outlet obstruction
• Gastrostomy and jejunostomy tubes
Balloon-tipped catheters should not be placed into small bowel (may obstruct lumen)
Small amount of free air after placement is common and usually does not require intervention
IMAGING
• Malposition is most frequent complication of feeding tubes
Can be visualized on chest or abdominal radiograph
Auscultation over abdomen is not reliable method for confirming proper tube placement
CLINICAL ISSUES
• 1-3% of feeding tubes enter tracheobronchial tree
Anywhere from trachea to pleural space
Can perforate lung with significant morbidity and mortality
• Tube may penetrate esophagus or duodenum with fatal results
Often through diverticula (e.g., Zenker), due to thin wall
• High-risk patients
Altered mental status
Absent gag reflex
Multiple or repetitive insertion attempts
• Treatment
Reposition feeding tube if in incorrect location
Perforation of lung or bowel may require surgery
(Left) Esophagram shows a retroesophageal collection of gas and contrast medium resulting from perforation of a Zenker diverticulum by attempted placement of a feeding tube whose track runs parallel to the proximal esophagus.
(Right) Chest radiograph shows a feeding tube that has entered the right bronchus and perforated the lung though a lower lobe bronchus. The tip lies in the pleural space, a procedural complication that may be fatal, especially if food is given through the tube.
(Left) Frontal radiograph shows the peculiar course of the feeding tube with abrupt upper deviation of its distal portion. CT showed that the tube had perforated the duodenum and had been advanced with its wire in place.
(Right) Axial CECT shows a feeding gastrostomy tube entering the stomach. The balloon tip of the tube has migrated into the jejunum where it is partially occluding its lumen.
TERMINOLOGY
Definitions
• Patient injury caused by improper feeding tube placement
• Feeding tubes
Small, soft enteric tubes
Some with flexible metallic tips
Used for feeding chronically ill patients
Can be used for long periods of time
• Nasogastric tubes
Large-bore, moderately stiff
Buy Membership for Radiology Category to continue reading. Learn more here

















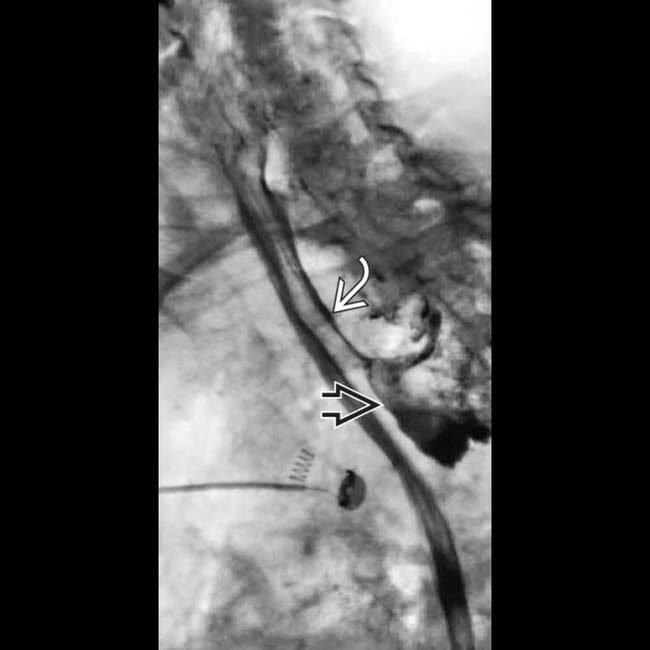
 resulting from perforation of a Zenker diverticulum by attempted placement of a feeding tube whose track
resulting from perforation of a Zenker diverticulum by attempted placement of a feeding tube whose track  runs parallel to the proximal esophagus.
runs parallel to the proximal esophagus.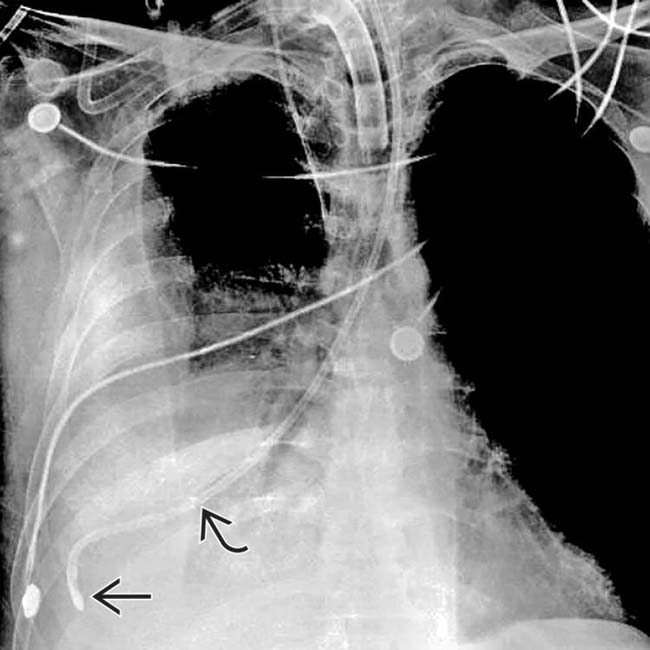
 that has entered the right bronchus and perforated the lung though a lower lobe bronchus. The tip
that has entered the right bronchus and perforated the lung though a lower lobe bronchus. The tip  lies in the pleural space, a procedural complication that may be fatal, especially if food is given through the tube.
lies in the pleural space, a procedural complication that may be fatal, especially if food is given through the tube.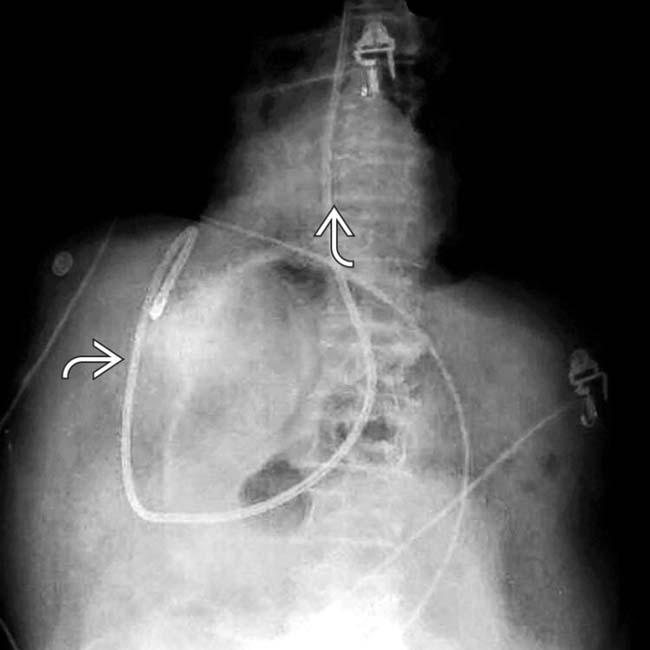
 with abrupt upper deviation of its distal portion. CT showed that the tube had perforated the duodenum and had been advanced with its wire in place.
with abrupt upper deviation of its distal portion. CT showed that the tube had perforated the duodenum and had been advanced with its wire in place.
 entering the stomach. The balloon tip of the tube
entering the stomach. The balloon tip of the tube  has migrated into the jejunum where it is partially occluding its lumen.
has migrated into the jejunum where it is partially occluding its lumen.






































 is evident.
is evident.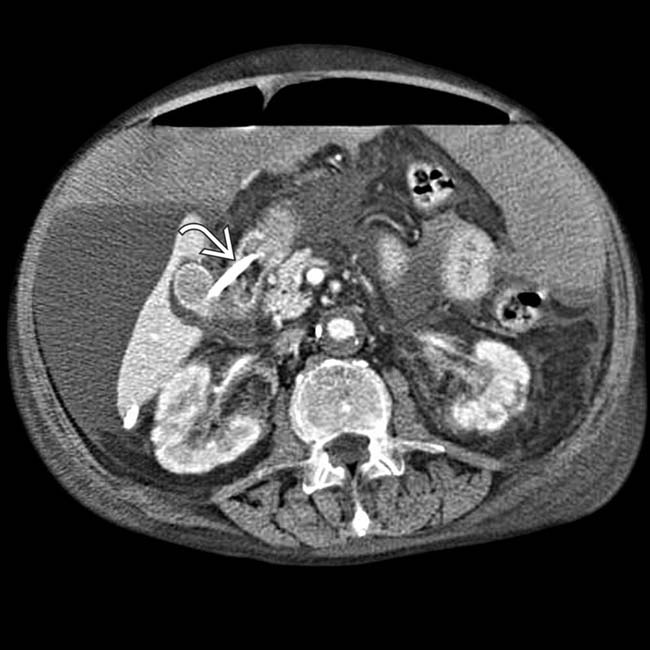
 .
.
 through the lateral wall of the duodenum is noted
through the lateral wall of the duodenum is noted  .
.
 free in the peritoneal cavity. Placement of tube feedings through this tube resulted in free intraperitoneal gas
free in the peritoneal cavity. Placement of tube feedings through this tube resulted in free intraperitoneal gas  and complex fluid.
and complex fluid.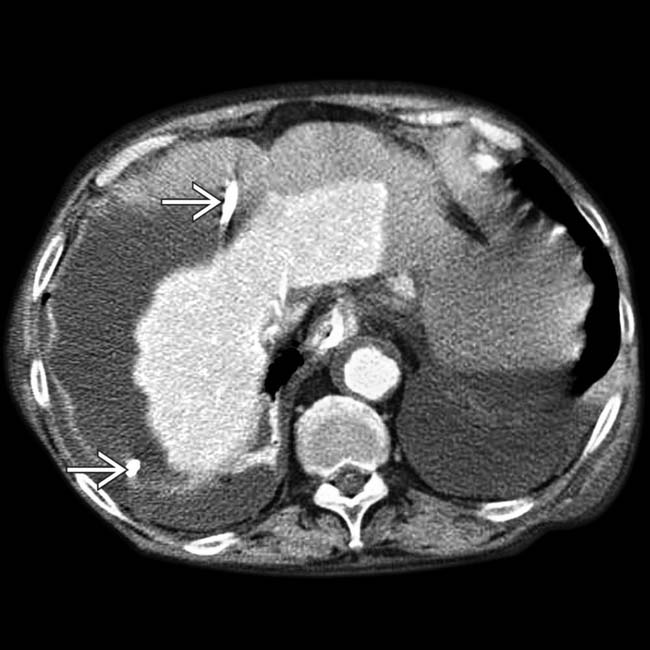
 is free in the peritoneal cavity.
is free in the peritoneal cavity.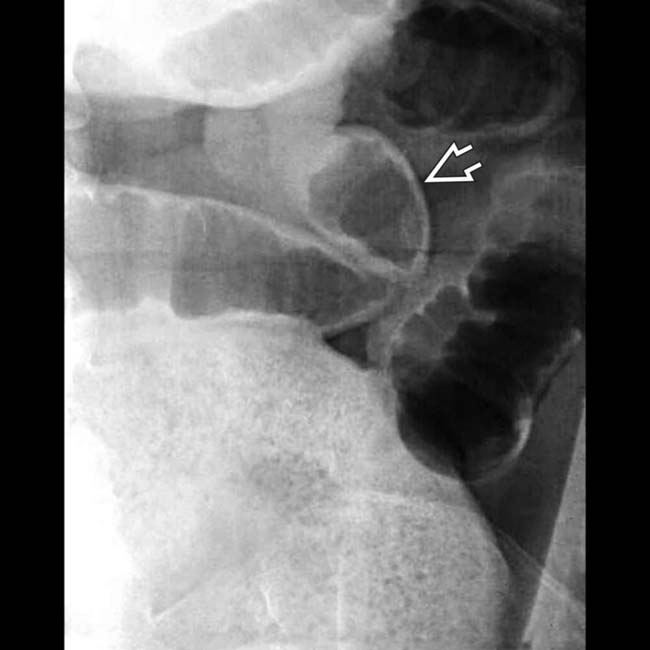
 , a well-recognized (Rigler) sign of pneumoperitoneum.
, a well-recognized (Rigler) sign of pneumoperitoneum.
 . Both the inside and outside of the bowel wall are seen
. Both the inside and outside of the bowel wall are seen  , a well-recognized (Rigler) sign of pneumoperitoneum. The external portion of the PEG tube is seen
, a well-recognized (Rigler) sign of pneumoperitoneum. The external portion of the PEG tube is seen  .
.