Hypogastric Artery Ligation
This operation is usually performed as an emergency procedure for postpartum hemorrhage in lieu of hysterectomy. It also may be performed for nonobstetric uncontrolled bleeding (e.g., postirradiation hemorrhage, vaginal laceration bleeding, cervical bleeding, posthysterectomy bleeding). Hypogastric ligation affects clotting by reducing ipsilateral pulse pressure (85% decrease) and blood flow (50% decrease).
The operation requires a laparotomy. The retroperitoneum is entered by opening the peritoneum above the external iliac artery over the psoas major muscle (Fig. 20–1). The external iliac artery and vein are exposed in the direction of the bifurcation of the common iliac artery (Fig. 20–2). As the dissection proceeds cranially, the ovarian vessels and the ureter are encountered as they cross the common iliac artery (Fig. 20–3). The external iliac artery is retracted with a vein retractor to expose the hypogastric artery (Fig. 20–4). A long right-angle clamp is used to carefully dissect a plane between the common hypogastric artery and its underlying vein (Fig. 20–5). Injury to the hypogastric vein(s) must be avoided at all costs because these large veins, deeply located in the pelvis, are exceedingly difficult to suture. By spreading and closing the clamp, the dissection can be quickly completed. A ligature of 0 Vicryl is passed through the tip of the right-angle clamp and pulled under the hypogastric artery (Fig. 20–6). The ureter is reidentified and observed not to be caught in the ligature. The ligature is then tied with three or four throws and cut (Figs. 20–7 and 20–8). The common and external iliac arteries are rechecked to ensure that only the correct vessel (i.e., the hypogastric artery) has been tied off. Additionally, it is advisable to examine the integrity of the hypogastric vein (Fig. 20–9). The peritoneum is closed with a 3-0 Vicryl running stitch. The procedure is repeated on the contralateral side.
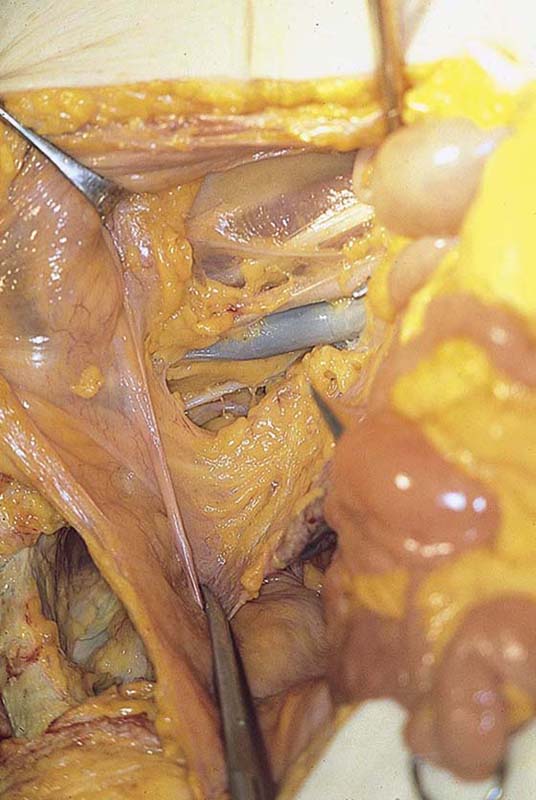
FIGURE 20–1 The peritoneum overlying the external iliac artery and the psoas major muscle has been opened, exposing the external iliac artery and vein.

FIGURE 20–2 The scissors are resting on the right external iliac vein.

FIGURE 20–3 The right ureter is identified as it crosses over the pelvic brim and the right common iliac artery.

FIGURE 20–4 Dissection is begun between the right hypogastric artery and vein with the use of a right-angle clamp. Care must be taken not to injure the underlying hypogastric vein.
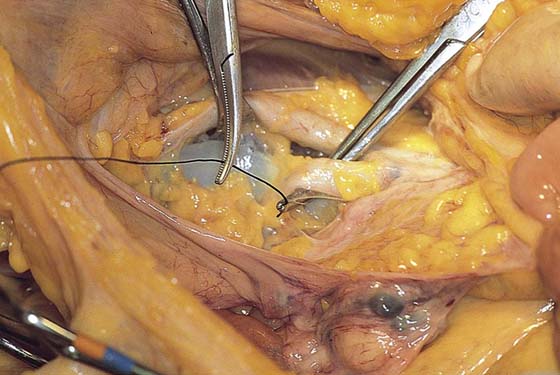
FIGURE 20–5 The clamp has created a plane between the hypogastric artery and vein. A ligature of 0 Vicryl is passed to the tip of the right-angle clamp.
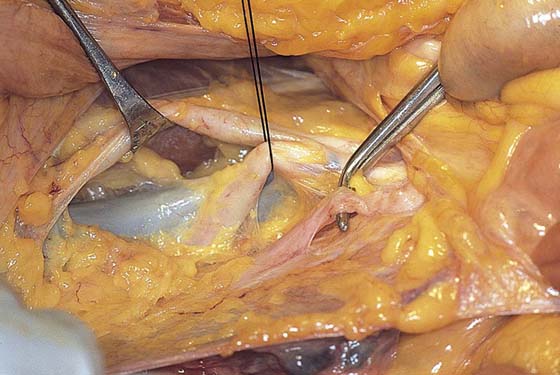
FIGURE 20–6 The ligature has been completely passed beneath the common hypogastric artery. The ends of the ligature have been grasped and traction applied to gently elevate the vessel. The right ureter is reidentified.
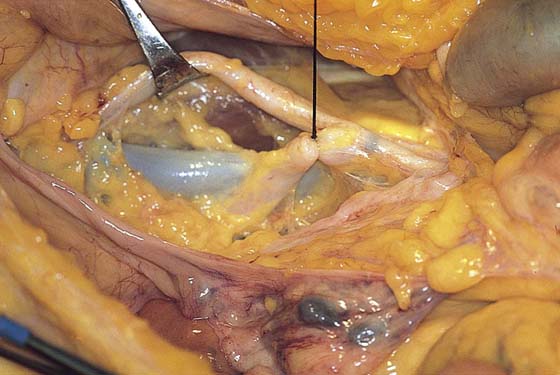
FIGURE 20–7 The ligature is secured with three throws. Each throw is tied down squarely. The external iliac artery is retracted with a vein retractor.

FIGURE 20–8 The ligature is cut.
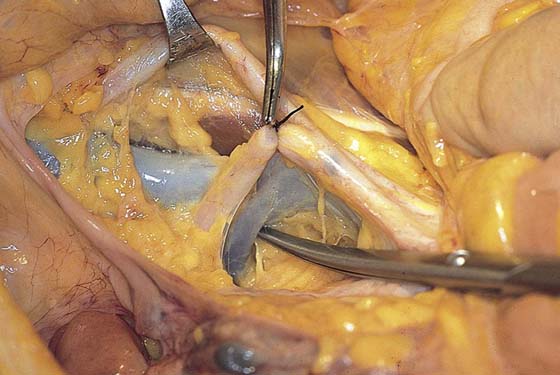
FIGURE 20–9 A final inspection is carried out to ensure that the common and external iliac arteries were not inadvertently ligated. Similarly (tip of scissors), the hypogastric vein is checked to ensure that it is intact.






