7 Hypertrophic Cardiomyopathy
Background
Overview of Echocardiographic Approach
Step-by-Step Approach to the Evaluation of HCM
Step 1: Establish the Diagnosis of HCM
Step 2: Exclude Other Causes of Increased Wall Thickness
Box 7-2 Differential Diagnosis of HCM on Echocardiography
Key Points
Athlete’s Heart3
Storage Diseases4
Key Points
Infiltrative Cardiomyopathies
Septal Hypertrophy in the Elderly
Step 3: Assess Pattern and Severity of Left Ventricular Hypertrophy
Key Points
Anatomic Imaging
Acquisition
Analysis
Key Points
Severity of Left Ventricular Hypertrophy
TABLE 7-1 EXTENT OF HYPERTROPHY ACCORDING TO ECHOCARDIOGRAPHIC POINT SCORE
| Extent of Hypertrophy | Points |
|---|---|
| Septal thickness, mm (basal third of septum) | |
| 15–19 | 1 |
| 20–24 | 2 |
| 25–29 | 3 |
| >30 | 4 |
| Extension to papillary muscles (basal two thirds of septum) | 2 |
| Extension to apex (total septal involvement) | 2 |
| Anterolateral wall extension | 2 |
| Maximum total | 10 |
Other Morphologic Subtypes of HCM
Apical HCM
Step 4: Determine if There Is LVOT Obstruction
Key Points
Step 4A: Assess for the Presence of LVOT Obstruction at Rest
Anatomic Imaging
Physiologic Data
Acquisition
Analysis
Key Points

where V is peak velocity in the LVOT.
Pitfalls
Step 4B: In Patients without Resting LVOT Obstruction, Determine if There Is Provocable LVOT Obstruction
Key Points
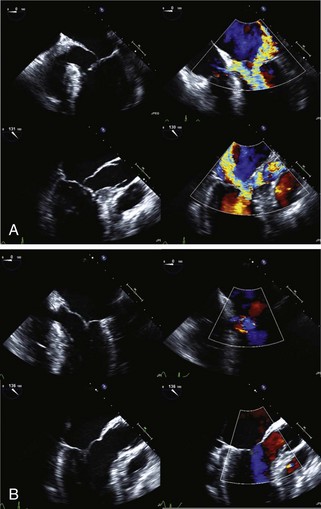
Step 5: Assess the Mechanism of Mitral Regurgitation
Step 6: Assess Left Ventricular Diastolic Function
Step 6A: Measure Diastolic Filling Parameters and Determine E/e′ Ratio
Key Points
Tissue Doppler Imaging
Acquisition
Analysis
Step 6B: Determine Left Atrial Volume
Acquisition

Step 7: Assess Left Ventricular Systolic Function
Step 7B: Assess Myocardial Mechanics
Key Points
Speckle Tracking Echocardiography (STE)
Step 8: Use Echocardiographic Data in the Management of Obstructive HCM
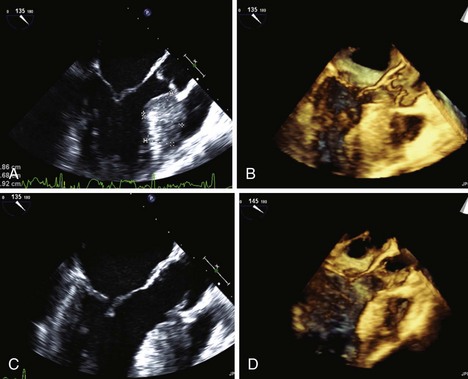
Septal Ethanol Ablation
Key Points
Surgical Myectomy
Key Points
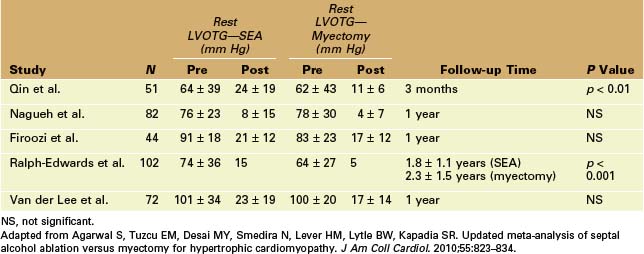
Selection of Invasive Septal Reduction Therapy
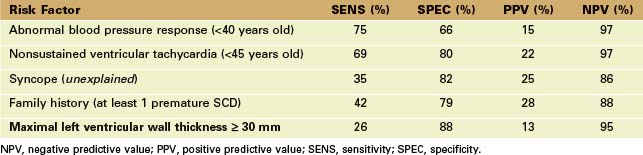
Key Measurements for Predicting Prognosis in Patients with HCM
Key Points
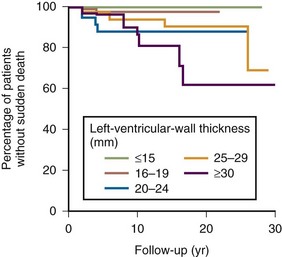
Left Ventricular Wall Thickness
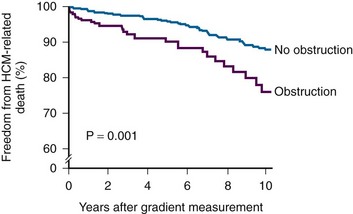
LVOT Obstruction
LV Systolic Dysfunction
Left Atrial Enlargement
Additional Testing in Patients with HCM
Exercise Testing and Exercise Echocardiography
Provocable LVOT Obstruction
Key Points
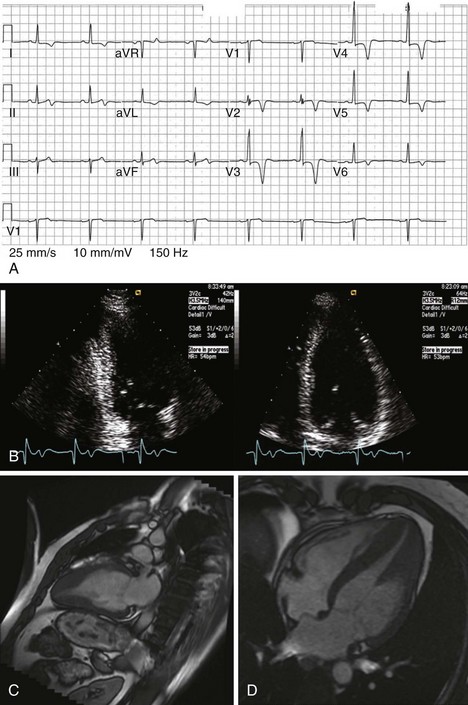
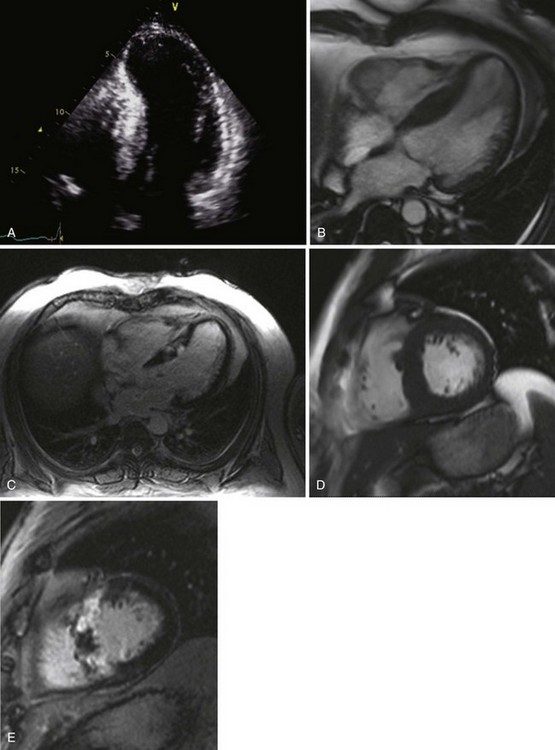
Cardiovascular Magnetic Resonance Imaging in HCM
Diagnosis of HCM and Characterization of Hypertrophy
Key Points
Identification of Fibrosis in HCM and Prognostication
1 Maron BJ, McKenna WJ, Danielson GK, et al. Clinical expert consensus document on hypertrophic cardiomyopathy: A report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents and the European Society of Cardiology Committee for Practice Guidelines. J Am Coll Cardiol. 2003;42:1687-1713.
2 Nagueh SF, Mahmarian JJ. Noninvasive cardiac imaging in patients with hypertrophic cardiomyopathy. J Am Coll Cardiol. 2006;48:2410-2422.
3 Maron BJ, Pelliccia A. The heart of trained athletes: Cardiac remodeling and the risks of sports, including sudden death. Circulation. 2006;114:1633-1644.
4 Arad M, Maron BJ, Gorham JM, et al. Glycogen storage diseases presenting as hypertrophic cardiomyopathy. N Engl J Med. 2005;352:362-372.
5 Lang RM, Bierig M, Devereux RB, et al. Recommendations for chamber quantification: A report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr. 2005;18:1440-1463.
6 Mulvagh SL, Rakowski H, Vannan MA, et al. American Society of Echocardiography Consensus Statement on the clinical applications of ultrasonic contrast agents in echocardiography. J Am Soc Echocardiogr. 2008;21:1179-1201.
7 Losi MA, Nistri S, Galderisi M, et al. Echocardiography in patients with hypertrophic cardiomyopathy: Usefulness of old and new techniques in the diagnosis and pathophysiological assessment. Cardiovasc Ultrasound. 2010;8:7.
8 Afonso LC, Bernal J, Bax JJ, Abraham TP. Echocardiography in hypertrophic cardiomyopathy: The role of conventional and emerging technologies. J Am Coll Cardiol Imag. 2008;1:787-800.
9 Agarwal S, Tuzcu EM, Desai MY, Smedira N, Lever HM, Lytle BW, Kapadia SR. Updated meta-analysis of septal alcohol ablation versus myectomy for hypertrophic cardiomyopathy. J Am Coll Cardiol. 2010;55:823-834.
10 Maron BJ, Dearani JA, Ommen SR, et al. The case for surgery in obstructive hypertrophic cardiomyopathy. J Am Coll Cardiol. 2004;44:2044-2053.
11 McKenna WJ, Behr ER. Hypertrophic cardiomyopathy: Management, risk stratification, and prevention of sudden death. Heart. 2002;87:169-176.
12 Spirito P, Bellone P, Harris KM, et al. Magnitude of left ventricular hypertrophy and risk of sudden death in hypertrophic cardiomyopathy. N Engl J Med. 2000;342:1778-1785.
13 Maron MS, Olivotto I, Betocchi S, et al. Effect of left ventricular outflow tract obstruction on clinical outcome in hypertrophic cardiomyopathy. N Engl J Med. 2003;348:295-303.
14 Salerno M, Kramer CM. Prognosis in hypertrophic cardiomyopathy with contrast-enhanced cardiac magnetic resonance: The future looks bright. J Am Coll Cardiol. 2010;56:888-889.
1 Maron BJ, Maron MS, Wigle ED, Braunwald E. The 50-year history, controversy, and clinical implications of left ventricular outflow tract obstruction in hypertrophic cardiomyopathy: From idiopathic hypertrophic subaortic stenosis to hypertrophic cardiomyopathy. J Am Coll Cardiol. 2009;54:191-200.
2 Drinko JK, Nash PJ, Lever HM, Asher CR. Safety of stress testing in patients with hypertrophic cardiomyopathy. Am J Cardiol. 2004;93:1443-1444.
3 Maron MS, Olivotto I, Zenovich AG, et al. Hypertrophic cardiomyopathy is predominantly a disease of left ventricular outflow tract obstruction. Circulation. 2006;114:2232-2239.
4 Nagueh SF, Appleton CP, Gillebert TC, et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography. J Am Soc Echocardiogr. 2009;22:107-133.
5 Wang J, Buergler JM, Veerasamy K, Ashton YP, Nagueh SF. Delayed untwisting: The mechanistic link between dynamic obstruction and exercise tolerance in patients with hypertrophic obstructive cardiomyopathy. J Am Coll Cardiol. 2009;54:1326-1334.
6 Yang H, Woo A, Monakier D, et al. Left atrial enlargement in hypertrophic cardiomyopathy: The importance of left ventricular segmental hypertrophy and diastolic dysfunction. J Am Soc Echocardiogr. 2005;18:1074-1082.
7 Serri K, Reant P, Lafitte M, et al. Global and regional myocardial function quantification by two-dimensional strain. J Am Coll Cardiol. 2006;47:1175-1181.
This paper is the first major study of 2D strain imaging in patients with HCM.
8 Elliott PM, Gimeno JR, Thaman R, et al. Historical trends in reported survival rates in patients with hypertrophic cardiomyopathy. Heart. 2006;92:785-791.
9 Maron BJ. Contemporary insights and strategies for risk stratification and prevention of sudden death in hypertrophic cardiomyopathy. Circulation. 2010;121:445-456.
10 Nagueh SF, Bierig M, Budoff MJ, et al. American Society of Echocardiography clinical recommendations for multimodality cardiovascular imaging of patients with hypertrophic cardiomyopathy. Endorsed by the American Society of Nuclear Cardiology, Society for Cardiovascular Magnetic Resonance, and Society of Cardiovascular Computed Tomography. J Am Soc Echocardiogr. 2011;24:473-498.