Chapter 10 Hypertension and stroke
EPIDEMIOLOGY AND AETIOLOGY
Hypertension or high blood pressure (BP) is a sustained rise in resting blood pressure. Persistent systolic blood pressure (≥ 140 mmHg) and diastolic blood pressure (≥ 90 mmHg) is considered ‘hypertension’.1 It is very common, affecting approximately one-third of the population. Hypertension is an important risk factor in coronary heart disease and in cerebrovascular accident or ‘stroke’, and may also lead to kidney failure and left ventricular failure or ‘heart failure’.2,3 Hypertension with no known cause (primary) is the most common (90%), and hypertension with an identified cause (secondary) can be due to kidney disease (the most common cause), coarctation of the aorta, endocrine diseases and pregnancy.1 Diagnosis is by sphygmomanometry, usually over three consecutive visits to a medical doctor.4
Left ventricular hypertrophy usually develops in response to some factor, such as high blood pressure, that requires the left ventricle to work harder. As the workload increases, the walls of the chamber grow thicker, lose elasticity and eventually may fail to pump with as much force as a healthy heart.5 Left ventricular hypertrophy presents with increased risk of heart disease, including heart attack, heart failure, irregular heartbeats (arrhythmia) and sudden cardiac arrest.6
The term ‘stroke’ encompasses a heterogenous group of cerebrovascular disorders. Ischaemic stroke or cerebral infarction accounts for 80–85% of all strokes and typically presents as a sudden, painless, focal neurological deficit with preserved consciousness.1,2 Haemorrhagic stroke accounts for 15–20% of all strokes, and presents as an acute focal neurological deficit, but continues to worsen as the haematoma expands, with headache and altered consciousness resulting.5
RISK FACTORS
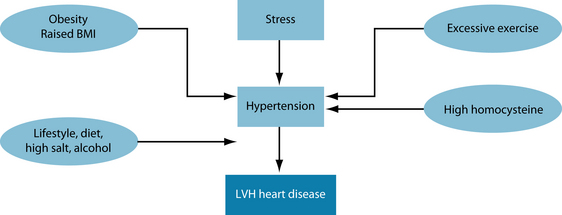
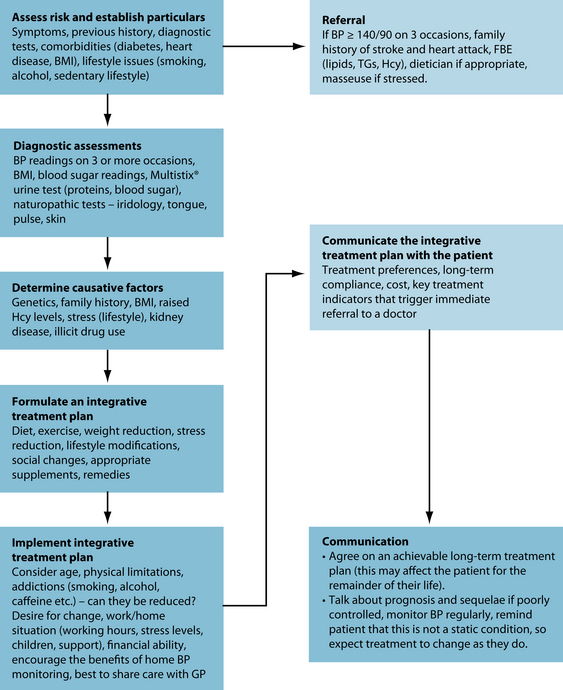
Genetics, social behaviour and diet all have a role to play in this multifactorial condition (see Figure 10.1).7 The risk of high blood pressure increases with age, and is more prevalent in middle-aged men and postmenopausal women.8 It develops at an earlier age in black ethnicity than it does in Caucasians and is influenced by family history. Although the long-term effect of stress on blood pressure is not well understood, chronic stress can lead to transient rises of significant hypertension.9 Dietary factors that may affect hypertension include high levels of salt, reduced levels of potassium, and heavy drinking. Apart from alcohol, other social behaviours such as smoking and physical inactivity have long-term detrimental effects on blood pressure.10
CONVENTIONAL TREATMENT
The initial medical treatment in non-life-threatening hypertension centres on weight loss and dietary changes.11 Patients are encouraged to increase the level of fruits and vegetables in their diet, while concurrently reducing salt and alcohol intake. These interventions, combined with regular aerobic exercise, can reduce systolic blood pressure by 6–10 mmHg.13
If the hypertension is high (> 140/90 mmHg) on several occasions or unresponsive to lifestyle modification, then drug therapy is instigated.1 For uncomplicated hypertension, unless there is a contraindication or a specific indication for another drug, then the order of consideration is:
For all patients, treatment aims to reduce BP to < 140/90 mm Hg; for those with a kidney disorder or diabetes, the goal is < 130/80 mm Hg or as near this level as tolerated. Even the elderly and frail can tolerate a diastolic BP as low as 60 to 65 mm Hg well without an increase in cardiovascular events.1
KEY TREATMENT PROTOCOLS
due to differences in the intake of certain nutrients. Sustained raised blood pressure is positively associated with higher sodium, alcohol and protein intakes, and is inversely associated with potassium, calcium and magnesium intake.13 Due to this, dietary and lifestyle measures are of primary focus in treating hypertension.
Stress reduction
The stress response increases sympathetic nervous activity, which can adversely affect the cardiovascular system (see Chapter 15 on adrenal fatigue). Cardiovascular disease is due in part to stress-induced mechanisms mediated primarily through increased adrenergic stimulation.5 These stress-induced mechanisms include elevations in serum lipids, alterations in blood coagulation, atherogenesis, vascular changes in hypertension and myocardial ischaemia.9
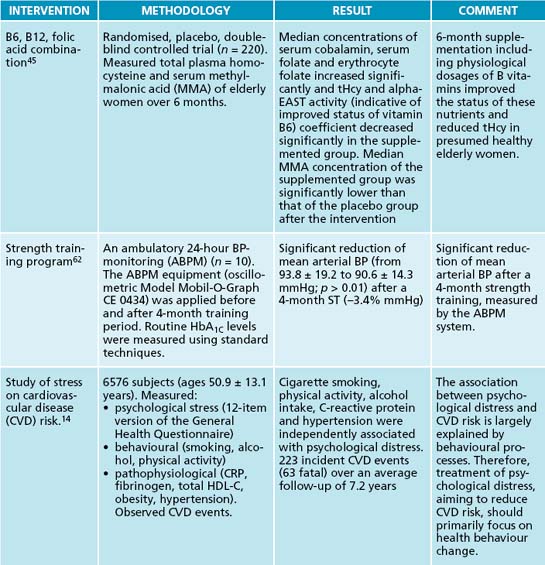
It is difficult to quantify the extent to which stress influences cardiovascular health; however, there are causal relationships between stress and pathophysiological behaviours that in turn have detrimental effects on health, including hypertension. A study over 7 years with 6576 subjects clearly indicated that stress led to increased consumption of alcohol, smoking and a reduction in physical activity.14 A small Indian study in 2008 of 77 individuals looked at the short-term effect of a comprehensive but brief lifestyle intervention with yoga on their subjective wellbeing. The group included healthy individuals as well subjects with hypertension, coronary artery disease and diabetes mellitus. The results suggested that the stress management program made an appreciable contribution to primary disease prevention.15
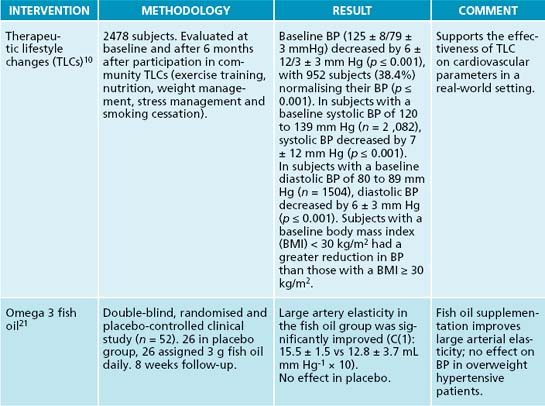
Interventions for coronary heart disease-prone behaviour patterns have proven successful. A large study was found to support the effect of therapeutic lifestyle changes on hypertension (see Table 10.2 at the end of the chapter for a review of the evidence).11 Valeriana officinalis may have a positive effect on anxiety and stress, as well as on vasospastic activity.16 It is believed that the relaxing effect of V. officinalis is related to the level of valerenic acid, a sesquiterpenic acid, which specifically modulates certain GABA-α receptors and activity.17 A 2007 study found ethanolic extracts of valerian to be as effective as nifedipine in their ‘anticoronaryspastic’ activity against cardiovascular disease.18 Another sesquiterpene isolated from Magnolia grandifolia flower petals produced a statistically significant decrease in coronary vascular resistance on the Langendorff isolated perfused heart.19 Passiflora incarnata was as effective as oxazepam in the treatment of generalised anxiety disorder, with low incidence of impairment of job performance20 (see Section 5 on the endocrine system and Section 4 on the nervous system).
Arterial elasticity and integrity
Age-related changes in the arterial system begin in the 1930s and accelerate through midlife.5 Increased collagen deposition and weakened vascular elastin result in altered elasticity, distensibility and dilatation.5 Stiffening of the central arteries results in higher wave velocities and augmentation of systolic arterial pressure.5 In a double-blind, randomised and placebo controlled clinical study, 26 overweight hypertensive patients were given 3 g of omega-3 fish oil daily for 8 weeks.21 After 8 weeks’ follow-up, the large artery elasticity in the fish-oil group, compared with its baseline, had significantly improved. A small study of 28 middle-aged men and women undertaking a randomised, double-blind trial of 400 IU of vitamin E daily for 8 weeks improved arterial compliance by 44% in 12 out of 14 subjects.22 Antioxidants, such as bioflavonoids, enhance endothelial nitric oxide (NO) synthase expression and subsequent NO release from endothelial cells; this is important in arterial vasodilation. Pycnogenol, an extract of bark from Pinus pinaster (French maritime pine) consists of a concentrate of water-soluble polyphenols. Pycnogenol contains the bioflavonoids catechin and taxifolin, as well as phenolcarbonic acids. Pycnogenol augments endothelium-dependent vasodilation by increasing NO production in the vascular wall.23
Dietary flavonoids, such as quercetin and epicatechin, can augment nitric oxide status and reduce endothelin-1 concentrations, and may thereby improve endothelial function.24 Cocoa is rich in plant-derived flavonoids. In the Zutphen Elderly Study, a cohort of 470 elderly men revealed that cocoa intake was inversely related to blood pressure. A small amount of dark chocolate daily (6 g) in the evening significantly reduced mean systolic blood pressure by 2.9 ± 1.6 mmHg and diastolic blood pressure by 1.9 ± 1.0 mmHg.25 Although still debated, a range of potential mechanisms through which flavonols and cocoa might exert their benefits on cardiovascular health include activation of NO and antioxidant anti-inflammatory and antiplatelet effects, which in turn might improve endothelial function, lipid levels, blood pressure, insulin resistance and eventually clinical outcome.25 It was also shown that homocysteine-lowering therapy improved small arterial elasticity in diabetic patients treated with high-dose metformin.26
Magnesium plays a role in a number of chronic disease-related conditions, including hypertension. Magnesium acts as a calcium channel antagonist, stimulates production of vasodilator prostacyclins and nitric oxide and alters vascular responses to vasoactive agonists.27 It may also play a role in metabolic syndrome and raised serum lipid profiles. Interestingly, it has a more profound effect when added to the diet than it does when supplemented.28
Most of the herbal treatments for hypertension probably act as peripheral vasodilators.1 One of the most useful herbs is Crataegus oxyacantha; its leaves, flowers and fruits contain such biologically active substances as flavonoids and catechins, which appear to be related to C. oxyacantha antioxidant effects.29 As well as reducing high blood pressure this herb has a trophic effect on heart muscle.31 Other studies have shown that C. oxyacantha reduces resting heart rate and mean diastolic blood pressure during exercise and increases the perfusion of the myocardium through revascularisation.29 This is important because left ventricular heart failure is often caused by prolonged hypertension.1 In a pilot study where 500 mg of Crataegus oxyacantha extract was taken daily for 10 weeks, there were promising results on the diastolic component of mild hypertension among subjects.30
Vasopressin and diuresis
Diuretics have long been used to treat hypertension in general practice. Technically, a ‘diuretic’ is an agent that increases urine volume, while a ‘natriuretic’ causes an increase in renal sodium excretion. Because natriuretics almost always also increase water excretion, they are usually called diuretics.31 Generally, diuretics should be initiated at the lowest effective dose of the class chosen. Problems that may occur with both short- and long-term use of diuretics include hyponatraemia, hypokalaemia, metabolic alkalosis and increased uric acid levels. Carbohydrate metabolism is frequently disturbed, with resultant hyperglycaemia and insulin resistance.32 A review of the scientific evidence associated with herbal diuretics showed promising results.31 One such herb that exhibits diuretic effects is Taraxacum officinale. It is important that the leaves are used, as they have high levels of potassium.31 The effect of an aqueous extract of Phyllanthus amarus administered intravenously on male normotensive rabbits produced a fall in mean diastolic, systolic and arterial pressure.33 Methyl brevifolincarboxylate isolated from the leaves of Phyllanthus niruri showed a vasorelaxant effect on rat aortic rings. It exhibited slow relaxation activity against norepinephrine-induced contractions of rat aorta with or without endothelium.34 A single oral administration of a 5% aqueous extract of Phyllanthus sellowianus (400 mg/kg body weight) produced significant increases in urinary excretion in test animals.35 Clerodendron trichotomum has been traditionally used for the treatment of hypertension in China, Korea and Japan. An ethanolic extract produced the following phenylpropanoid glycosides: acteoside, leucosceptoside A, martynoside, acteoside isomer and isomartynoside. These glycosides displayed significant angiotensin-converting enzyme inhibition.36
Body mass index
Obesity and hypertension are highly correlated;37 however, the concept of ideal body weight may raise more questions than it answers. The body mass index (BMI) attempts to create a statistical framework that can be used as a clinical tool to assess ‘normal, healthy’ human weight. While the method may provide an understanding of ideal weight for individuals of varying heights, it does not take into account muscle mass and body frame.
The body mass index (BMI) is a ratio:
| BMI (KG/M2) | WEIGHT CATEGORY |
|---|---|
| Less than 18.5 | Underweight |
| 18.5 to 24.9 | Healthy |
| 25 to 29.9 | Overweight |
| 30 or higher | Obese |
Source: ‘Understanding body mass index’.38
In the Physician’s Health Study,37 raised BMI over an 8-year period correlated with an increased risk of cardiovascular disease in 13,230 middle-aged men. Women are not immune to the effects of BMI on hypertension. Caucasian women with a BMI > 30 kg/m2 had a significantly greater risk of CVD mortality than women with a ‘normal’ BMI.39 This was particularly so in women below the age of 60 years.39 A BMI > 30 plus any two of triglycerides ≥ 1.7 mmol/L, HDL < 1.03, BP ≥ 130/85 mmHg and fasting glucose ≥ 5.6 mmol/L is considered to be metabolic syndrome40 (discussed further in Chapter 16 on diabetes). As there is a continuous linear relationship between excess body fat blood pressure and the prevalence of hypertension,31 weight loss to achieve normal BMI should always be attempted.
Homocysteine (Hcy)
As mentioned previously, over-exercise as well as deficiency of folic acid, vitamin B6 and/or vitamin B12 can result in elevated total plasma homocysteine concentrations (tHcy), which is considered to be a risk factor for vascular disease.41 As discussed in Chapter 9 on atherosclerosis, there is considerable evidence to suggest that Hcy plays a significant role in the pathology of cardiovascular disease. Elevated levels of Hcy may be related to the cause of isolated systolic hypertension in some individuals, and in normotensive older adults is an independent risk factor for atherosclerosis.41 Some antihypertensive medications, such as candesartan and amlodipine, were effective in reducing cellular oxidative stress, but this effectiveness was reduced when the patient also had raised Hcy levels.42 Experimentally increasing plasma Hcy concentrations by methionine loading rapidly impairs both conduit and resistance vessel endothelial function in healthy humans. Endothelial dysfunction in conduit and resistance vessels may underlie the reported associations between Hcy, atherosclerosis and hypertension. Increased oxidant stress appears to play a pathophysiological role in the deleterious endothelial effects of Hcy.43
A ‘healthy’ vegetarian diet may be considered a healthy choice for hypertensive individuals, due to its effect on the reduction of saturated fats and general beneficial effects on weight. However 66% of vegans and vegetarians in a group of Austrian cohorts had considerably lower levels of vitamins B2 and B12; these led to excessive levels of Hcy.44 Raised Hcy levels can be relatively easily reduced by daily supplementation of vitamins B6 and B12 and folate.45
Prevention and treatment of stroke
A great concern of chronic hypertension is stroke.5 Ginkgo biloba, a Chinese traditional medicine, is widely used in the treatment of acute ischaemic stroke in China.46 Its efficacy, however, is uncertain. A Cochrane review of 10 trials produced mixed results.47 Whereas it has been shown that G. biloba extract leads to a significant increase in cerebral blood flow and glucose uptake into brain tissue, there was no convincing evidence, from trials of sufficient methodological quality, to support the routine use of G. biloba to promote recovery after stroke.47 A more recent trial in wild mice produced more encouraging results. A Ginkgo extract, EGb761, administered orally to mice produced 50.9% less neurological dysfunction and 48.2% smaller infarct volumes than non-treated mice after cerebral infarct (stroke).48 Part of the positive result was attributed to its ability to induce haem oxygenase.48 It is interesting to note that a recent study examining the effects of a G. biloba extract on the distal left anterior descending coronary artery blood flow and plasma nitric oxide and endothelin-1 levels in patients with coronary artery disease produced encouraging results. The treatment led to an increase of artery blood flow as well as an alteration in the nitric oxide/endothelin-1 ratio, which produced a beneficial result.49
There is evidence to support the use of acupuncture in stroke victims. Issues such as spasticity and anxiety are commonplace amongst sufferers. Poststroke anxiety neurosis was successfully relieved with acupuncture in 82.35% of patients in a small trial of 34 individuals.50 A trial of 131 patients with spastic hemiplegia received two 30-day treatment regimens involving traditional acupuncture treatment.51 Acupuncture was effective in reducing spastically increased muscle tone and motor neuron excitability in spastic hemiplegia and could improve spastic states in stroke patients. A study in the poststroke rehabilitation wards of five UK hospitals using acupuncture with electrical stimulation over 4 weeks produced a negative result, with acupuncture failing to produce a benefit over placebo.52 A Cochrane review of 31 trials involving the organised inpatient care for stroke victims indicated that patients who receive this care are more likely to survive their stroke, return home and become independent in looking after themselves.53 While current evidence is not entirely supportive, more study needs to be done in this area to ascertain if there is a role for complementary medicines in managing or preventing stroke.
INTEGRATIVE MEDICAL CONSIDERATIONS
The influence of stress in cardiovascular disease should not be underestimated. In fact it has been shown in clinical trials that unchecked long-term stress can be a contributing factor in hypertension.54 Massage therapists have suggested that their therapy elicits the relaxation response and therefore can decrease BP and hypertension.54 This is also dependent upon the type of massage, having greatest effect with relaxing (Swedish) massage.55 Regular massage therapy has been shown to reduce long-term hypertension. If the individual’s stress stems from environmental factors (such as work, home life, and financial problems), then referral to a counsellor or psychologist may be a consideration. Some patients may prefer to obtain dietary advice from a dietician or a qualified nutritionist.
Practitioners may also consider referral to an acupuncturist. However, a review of randomised clinical trials (RCTs) produced inconclusive results for this therapy, and revealed most studies to have poor methodology and small sample sizes.56 There is some evidence to suggest that acupuncture increases circulation by increasing the number of capillaries, thereby improving capillary density, decreasing venous and arterial blood stasis as well as reducing blood viscosity and haematocrit, resulting in improved circulation through the reduction of peripheral resistance.29 Acupuncture is also thought to decrease the rate of renin secretion by the kidneys.29 Yoga, an integral part of Ayurveda, has been shown to be useful to patients with heart disease and hypertension.57 Yoga may reduce anxiety, promote wellbeing and improve quality of life. Its safety profile is solid, but its use as a complementary therapeutic regimen under medical supervision may still be appropriate.30 Tai chi or other gentle martial art forms for stress reduction and general wellbeing may also be beneficial.
Example treatment
Prescription
The herbal formula is designed to exert a hypotensive action via smooth muscle relaxation, vasodilation and stress reduction (Valeriana spp., and Crataegus oxyacantha).31,17,29 Magnesium also indirectly produces vasodilation.27 A diuretic effect may occur via Taraxacum officinale.31 Ginkgo biloba may be of benefit in improving circulation and enhancing vascular integrity.47–49 Omega-3 fish oil can be taken at a dose of 6 capsules daily (1000 mg fish oil per capsule), to increase arterial elasticity.21 Vitamin B6 in a daily dose of 100 mg daily and vitamin B12 in a dose of 1000 μg daily will assist healthy homocysteine metabolism.41,44,45 It may be appropriate to use a sublingual form of B12 to overcome the low levels of intrinsic factor that may preclude gut absorption. Folic acid can be taken in
Dietary and lifestyle modifications
Diet
Naturopaths may consider embracing the findings of the Dietary Approaches to Stop Hypertension (DASH) Collaborative Research Group. In this study of 459 adults, groups were assigned one of two diets for 8 weeks.58 The first included raised levels of fruit and vegetables, and the second a combined diet, which was the same diet with added low-fat dairy products and reduced total fat. The group eating more fruit and vegetables had reductions of 2.8 mmHg (systolic) and 1.1 mmHg (diastolic). The group on the combined diet had even greater reductions of 5.5 mmHg (systolic) and 3 mmHg (diastolic).58 It is assumed that salt plays an important role in the inactivation of nitric oxide synthase in endothelial cells of arteries, causing a reduction in elasticity and an increase in pressure.59 Females of an older age are the most sensitive to the hypertensive effects of dietary sodium, so sodium consumption should be monitored in this population.60 Although the effects of caffeine on BP are considered to be temporary, a reduction in caffeine intake may be beneficial.
Exercise
There is strong epidemiological and experimental evidence to support a positive link between the lowering of BP and exercise. Aerobic exercise that uses large muscle groups for 20–60 minutes a day for a minimum of 3 days a week is advisable.1 It is interesting to note, however, that exercise over 758 minutes a week (108 minutes per day) increases methionine metabolism, which also increases its amino acid metabolic intermediate homocysteine (Hcy), known to increase cardiovascular risk.61 Strength training has also been shown to reduce arterial blood pressure in a small study of 10 participants with type 2 diabetes co-morbidity.62
Expected outcomes and follow-up protocols
The measurable outcomes that have the greatest influence on treatment regimen are:
The patient in this case is already in contact with a medical practitioner, and given his family history it would be prudent to ensure that he maintains his contact and has regular blood test reviews. This is especially important since he is overweight and has a family history of stroke, which is usually associated with dyslipidaemia. The patient is strongly advised to reduce his weight to a healthier level and stop smoking. He also needs to adopt an exercise program, which will have beneficial effects on both his weight and stress.
Of the subjective outcomes, those associated with satisfaction of treatment and reduction in stress, as well as with feelings of empowerment, are the most significant to take note of. After an initial consultation it would then be prudent to have a weekly follow-up for a month, then fortnightly return visits for another month, then four more monthly visits. At this 6-month point of treatment, if there are encouraging signs that there has been significant weight loss (assume an average of 0.5–1 kg/month) and good blood pressure control (BP ≤ 130/80 in ≥ 80% of monitor readings), then follow-up consultations could be extended to 6 months between visits.
Appel L.J., et al. A clinical trial of the effects of dietary patterns on blood pressure. DASH Collaborative Research Group. N Engl J Med. 1997;336(16):1117-1124.
Chang Q., et al. Hawthorn. J Clin Pharmacol. 2002;42(6):605-612.
Lawes C.M., et al. Blood pressure and coronary heart disease: a review of the evidence. Semin Vasc Med. 2002;2(4):355-368.
Mahady G.B. Ginkgo biloba for the prevention and treatment of cardiovascular disease: a review of the literature. J Cardiovasc Nurs. 2002;16(4):21-32.
1. The Merck Manual’s online medical library. Online. Available: http://www.merck.com/mmpe/sec07/ch071/ch071a.html. Accessed 28 September 2008.
2. Easton J.D., et al. Definition and evaluation of transient ischemic attack: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on Peripheral Vascular Disease. The American Academy of Neurology affirms the value of this statement as an educational tool for neurologists. Stroke. 2009;40(6):2276-2293.
3. Vardaxis N.J. Pathology for the health sciences. South Melbourne: MacMillan Education Australia; 1996. 106
4. Padwal R.S., et al. The 2009 Canadian Hypertension Education Program recommendations for the management of hypertension: part 1 – blood pressure measurement, diagnosis and assessment of risk. Can J Cardiol. 2009;25(5):279-286.
5. Textbook of cardiovascular medicine. Online. Available: http://ovidsp.tx.ovid.com. Accessed 15 February 2009.
6. The Mayo Clinic. Online. Available: http://www.mayoclinic.com/health/left-ventricular-hypertrophy/DS00680. Accessed 1 November 2008.
7. Murphy B.P., et al. Hypertension and myocardial ischemia. Med Clin North Am. 2009;93(3):681-695.
8. The Mayo clinic. Online. Available: http://www.mayoclinic.com/health/high-blood-pressure/DS00100/DSECTION = risk-factors. Accessed 5 October 2008.
9. Engler M.B., Engler M.M. Assessment of the cardiovascular effects of stress. J Cardiovasc Nurs. 1995;10(1):51-63.
10. Bavikati V.V., et al. Effect of comprehensive therapeutic lifestyle changes on prehypertension. Am J Cardiol. 2008;102(12):1677-1680.
11. Khan N.A., et al. The 2009 Canadian Hypertension Education Program recommendations for the management of hypertension: part 2 – therapy. Can J Cardiol. 2009;25(5):287-298.
12. Australian Medicines Handbook. Online. Available: http://amh.hcn.net.au/view.php. Accessed 15 April 2009.
13. Suter P., et al. Nutritional factors in the control of blood pressure and hypertension. Nutr Clin Care. 2002;5(1):9-19.
14. Hamer M., et al. Psychological distress as a risk factor for cardiovascular events: pathophysiological and behavioural mechanisms. J Am Coll Cardiol. 2008;52(25):2163-2165.
15. Sharma R., et al. Effect of yoga based lifestyle intervention on subjective wellbeing. Indian J Physiol Pharmacol. 2008;52(2):123-131.
16. Sarris J. Herbal medicines in the treatment of psychiatric disorders: a systematic review. Phytother Res. 2007;21(8):703-716.
17. Trauner G., et al. Modulation of GABAA receptors by valerian extracts is related to the content of valerenic acid. Planta Med. 2008;74(1):19-24.
18. Circosta C., et al. Biological and analytical characterization of two extracts from Valeriana officinalis. J Ethnopharmacol. 2007;112(2):361-367.
19. Del Valle-Mondragon, et al. Coronary vasodilator activity of vulgarenol, a sesquiterpene isolated from Magnolia grandiflora, and its possible mechanism. Phytother Res. 2009;23(5):666-671.
20. Akhondzadeh S., et al. Passionflower in the treatment of generalized anxiety: a pilot double-blind randomized controlled trial with oxazepam. J Clin Pharm Ther. 2001;26(5):363-367.
21. Wang S., et al. Fish oil supplementation improves large arterial elasticity in overweight hypertensive patients. Eur J Clin Nutr. 2008;62(12):1426-1431.
22. Mottram P., et al. Vitamin E improves arterial compliance in middle-aged men and women. Atherosclerosis. 1999;145(2):399-404.
23. Nishioka K., et al. Pycnogenol, French maritime pine bark extract, augments endothelium-dependent vasodilation in humans. Hypertension Res. 2007;30(9):775-780.
24. Loke W.M., et al. Pure dietary flavonoids quercetin and (–)–epicatechin augment nitric oxide products and reduce endothelin-1 acutely in healthy men. Am J Clin Nutr. 2008;88(4):1018-1025.
25. Corti R., et al. Cocoa and cardiovascular health. Circulation. 2009;119:1433-1441.
26. Mashavi M., et al. Effect of homocysteine-lowering therapy on arterial elasticity and metabolic parameters in metformin-treated diabetic patients. Atherosclerosis. 2008;199(2):362-367.
27. Sontia B., Touyz R.M. Magnesium transport in hypertension. Pathophysiology. 2007;14(3–4):205-211.
28. Champagne C. Magnesium in hypertension, cardiovascular disease, metabolic syndrome, and other conditions: a review. Nutr Clin Pract. 2008;23(2):142-151.
29. Sutherland J.A. Selected complementary methods and nursing care of the hypertensive patient. Holist Nurs Pract. 2001;15(4):4-11.
30. Walker A.F., et al. Promising hypotensive effect of hawthorn extract: a randomized double-blind pilot study of mild, essential hypertension. Phytotherapy Res. 2002;16(1):48-54.
31. Katzung, BG. Basic and clinical pharmacology. 10th edn. 2007. Online. Available: http://online.statref.com/Document/Document.aspx?docAddress = TlFOA7l8O5e5XA5c4bAs3A%3d%3d&Scroll = 1&Index = 0&SessionId = F5A72EKGPYHLJMJM. Accessed 30 May 2009.
32. Topol EJ, ed. Textbook of cardiovascular medicine. 3rd edn. 2007. Online. Available: http://ovidsp.tx.ovid.com/spa/ovidweb.cgi?&S = ELFHFPFONJDDONNMNCFLDFPJPKDHAA00&Link + Set = S.sh.18%7c1%7csl_10. Accessed 30 May 2009.
33. Amaechina F.C., Omogbai E.K. Hypotensive effect of aqueous extract of the leaves of Phyllanthus amarus Schum and Thonn (Euphorbiaceae). Acta Pol Pharm. 2007;64(6):547-552.
34. Iizuka T., et al. Vasorelaxant effects of methyl brevifolincarboxylate from the leaves of Phyllanthus niruri. Biol Pharm Bull. 2006;29(1):177-179.
35. Hnatyszyn O., et al. Diuretic activity of an aqueous extract of Phyllanthus sellowianus. Phytomedicine. 1999;6(3):177-179.
36. Kang D.G., et al. Angiotensin converting enzyme inhibitory phenylpropanoid glycosides from Clerodendron trichotomum. J Ethnopharmacol. 2003;89(1):151-154.
37. Bowman T.S., et al. Eight-year change in body mass index and subsequent risk of cardiovascular disease among healthy non-smoking men. Prev Med. 2007;45(6):436-441.
38. AccessMedicine. Understanding body mass index. Postgraduate Medicine;117(2). Online. Available: http://www.accessmedicine.com/patientEd.aspx?aID = 857710&searchStr = body+mass+index+procedure. Accessed 25 February 2009.
39. Abell J.E., et al. Age and race impact the association between BMI and CVD mortality in women. Public Health Rep. 2007;122(4):507-512.
40. Longmore, et al. Oxford handbook of clinical medicine, 7th edn. Oxford: Oxford University Press; 2007. 198
41. Sutton-Tyrrell K., et al. High homocysteine levels are independently related to isolated systolic hypertension in older adults. Circulation. 1997;96(6):1745-1749.
42. Muda P., et al. Effect of antihypertensive treatment with candesartan or amlodipine on glutathione and its redox status, homocysteine and vitamin concentrations in patients with essential hypertension. J Hypertension. 2005;23(1):105-112.
43. Kanani P.M., et al. Role of oxidant stress in endothelial dysfunction produced by experimental hyperhomocyst(e)inemia in humans. Circulation. 1999;100(11):1161-1168.
44. Majchrzak D., et al. B-vitamin status and concentrations of homocysteine in Austrian omnivores, vegetarians and vegans. Ann Nutr Metab. 2006;50(6):485-491.
45. Wolters M., et al. Effect of multivitamin supplementation on the homocysteine and methylmalonic acid blood concentrations in women over the age of 60 years. Eur J Nutr. 2005;44(3):183-192.
46. Di Renzo G. Ginkgo biloba and the central nervous system. Fitoterapia. 2000;71(Suppl. 1):S43-S47.
47. Zeng X., et al. Ginkgo biloba for acute ischaemic stroke. Cochrane Database Syst Rev. (4):2005;. CD003691. Online. Available: doi: 10.1002/14651858.CD003691.pub2
48. Saleem S., et al. Ginkgo biloba extract neuroprotective action is dependent on heme oxygenase 1 in ischemic reperfusion brain injury. Stroke. 2008;39(12):3389-3396.
49. Wu Y.Z., et al. Ginkgo biloba extract improves coronary artery circulation in patients with coronary artery disease: contribution of plasma nitric oxide and endothelin-1. Phytother Res. 2008;22(6):734-739.
50. Wu P., Liu S. Clinical observation on post-stroke anxiety neurosis treated by acupuncture. J Tradit Chin Med. 2008;28(3):186-188.
51. Zhao J.G., et al. Effect of acupuncture treatment on spastic states of stroke patients. J Neurol Sci. 2009;276(1–2):143-147.
52. Hopwood V., et al. Evaluating the efficacy of acupuncture in defined aspects of stroke recovery: a randomised, placebo controlled single blind study. J Neurol. 2008;255(6):858-866.
53. Stroke Unit Trialists’ Collaboration. Organised inpatient (stroke unit) care for stroke. Cochrane Database Syst Rev. (4):2007;. CD000197. Online. Available: doi: 10.1002/14651858.CD000197.pub2
54. Olney C.M. The effect of therapeutic back massage in hypertensive persons: a preliminary study. Biol Res Nurs. 2005;7(2):98-105.
55. Camron J.A., et al. Changes in blood pressure after various forms of therapeutic massage: a preliminary study. J Altern Complement Med. 2006;12(1):65-70.
56. Lee H., et al. Acupuncture for lowering blood pressure: systematic review and meta-analysis. Am J Hypertens. 2009;22(1):122-128.
57. Mamtani R., Mamtani R. Ayurveda and yoga in cardiovascular disease. Cardiol Rev. 2004;12(5):155-162.
58. Appel L.J., et al. A clinical trial of the effects of dietary patterns on blood pressure. DASH Collaborative Research Group. N Engl J Med. 1997;336(16):1117-1124.
59. Li J., et al. Salt inactivates endothelial nitric oxide synthase in endothelial cells. J Nutr. 2009;139(3):447-451.
60. He J., et al. Gender difference in blood pressure responses to dietary sodium intervention in the GenSalt study. J Hypertens. 2009;27(1):48-54.
61. Joubert L.M., Manore M.M. The role of physical activity level and B-vitamin status on blood homocysteine levels. Med Sci Sports Exerc. 2008;40(11):1923-1931.
62. Strasser B., et al. The benefit of strength training on arterial blood pressure in patients with type 2 diabetes mellitus measured with ambulatory 24-hour blood pressure systems. Wien Med Wochenschr. 2008;158(13–14):379-384.