[level-membership-for-internal-medicine-category]
Hypertension
Hypertension is the elevation of blood pressure. An individual is classified as hypertensive when there is a sustained rise in blood pressure to more than 140/90 mmHg on three or more readings, each at least one week apart. Most patients have essential hypertension and an underlying cause is identified in less than 10%.
Causes
Renal
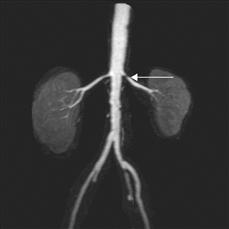
Figure 35 MRA renal arteries.
The patient presented with poorly-controlled hypertension. Subsequent examination revealed a bruit inferior to the left costal margin. MRA revealed a tight stenosis close to the origin of the left renal artery (arrow). The stenosis was successfully treated with angioplasty and stenting.
Drugs
History
Patients with uncomplicated essential hypertension are asymptomatic and are identified only in the course of routine physical examination; however, patients with secondary hypertension may complain of symptoms from the underlying disorder.
Patients with chronic pyelonephritis may have experienced recurrent urinary tract infections, with loin pain, pyrexia and rigors or have a history of childhood urinary tract infections or prolonged enuresis. Hypertension can also complicate glomerular disease; in particular it is associated with acute nephritic syndrome. Patients with nephritic syndrome may have experienced an acute illness with fatigue, malaise, haematuria, oliguria and oedema.
With Conn’s syndrome, patients may complain of muscle weakness and fatigue due to hypokalaemia and polyuria from impaired urine-concentrating ability. Paroxysms of headache, sweating, palpitations with flushing may be experienced by patients with phaeochromocytoma. Classically, these patients have attacks of hypertension; however, in the majority, the hypertension is sustained.
Weight gain, hair growth, acne, abdominal striae, muscle weakness, back pain and depression may be some of the symptoms experienced by patients with Cushing’s syndrome. With acromegaly, patients may complain of headaches, galactorrhoea, deepening of the voice, muscle weakness and joint pains. Hats and rings may no longer fit due to increasing size of the cranium and hands.
A complete drug history will identify offending drugs that may precipitate hypertension.
Examination
Inspection
On inspection, patients with acromegaly may have thick greasy skin, large hands, feet and tongue. Prominent supraorbital ridging with a large nose and protruding jaw accompanied by interdental separation may be noted on close inspection of the face and teeth. Confrontational testing of the visual fields may reveal bitemporal hemianopia, which may also be present with Cushing’s syndrome owing to compression of the optic chiasma by a pituitary adenoma. Additional features of Cushing’s disease include truncal obesity, acne, moon-like facies, bruising, striae, kyphosis and proximal muscle weakness.
Palpation and auscultation
In coarctation of the aorta, radiofemoral delay may be appreciated with simultaneous palpation of the radial and femoral arteries; bruits may be auscultated across collateral blood vessels along the axilla, chest wall and scapula. A systolic bruit may also be auscultated over the fourth left posterior intercostal space. Wide discrepancy of measured blood pressure may exist between the arm and leg.
Palpation of the abdomen may reveal bilateral ballotable masses due to enlarged polycystic kidneys, and bruits may be auscultated over stenosed renal arteries.
General Investigations
■ Urinalysis
Dipstick may indicate the presence of blood and protein. Urine microscopy is necessary to confirm the presence of red blood cells and also casts.
■ U&Es
Levels of serum potassium may be reduced with Conn’s syndrome due to hyperaldosteronism. High levels of creatinine and urea are found with renal failure.
■ Blood glucose
Atherosclerosis, renal vascular disease and nephropathy may be associated with diabetes. All of these may contribute to hypertension. Moreover conditions such as Cushing’s syndrome, acromegaly and phaeochromocytoma are associated with hyperglycaemia.
■ Serum lipids
Serum lipid estimation is used to screen for risk factors for atherosclerosis, and therapy may be initiated for the prevention of cerebrovascular and ischaemic heart disease.
■ ECG
A 12-lead ECG is recommended for all patients to provide a baseline and screen for left ventricular hypertrophy, which may result as a complication of hypertension.
Specific Investigations
■ Autoantibodies
Anti-GBM and ANCA may be positive with glomerulonephritis. ANA for connective tissue diseases.
■ Plasma catecholamines
Elevated in phaeochromocytoma.
■ Urinary catecholamines, metanephrines and vanillylmandelic acid
Elevated in phaeochromocytoma.
■ 24-hour urinary free cortisol
Excess cortisol in Cushing’s syndrome.
■ Low-dose dexamethasone suppression test
Failure of suppression of cortisol occurs in Cushing’s syndrome.
■ Oral glucose tolerance test
Failure of suppression of serum growth hormone occurs in acromegaly.
■ Plasma renin and aldosterone
Hypersecretion of aldosterone in the presence of low plasma renin levels confirms autonomous secretion in Conn’s syndrome.
■ Pregnancy test
Hypertension occurring with pre-eclampsia and eclampsia.
■ US abdomen
Polycystic kidneys. Duplex Doppler can screen for renal artery stenosis.
■ Renal angiography
Renal artery stenosis.
■ Renal biopsy
Renal causes of hypertension.
■ MRA
This is increasingly useful in the diagnosis of renal artery stenosis and avoids the need for potentially nephrotoxic radiocontrast administration.
[/level-membership-for-internal-medicine-category][not-level-membership-for-internal-medicine-category]
Hypertension
Hypertension is the elevation of blood pressure. An individual is classified as hypertensive when there is a sustained rise in blood pressure to more than 140/90 mmHg on three or more readings, each at least one week apart. Most patients have essential hypertension and an underlying cause is identified in less than 10%.
Causes
Renal
Figure 35 MRA renal arteries.
The patient presented with poorly-controlled hypertension. Subsequent examination revealed a bruit inferior to the left costal margin. MRA revealed a tight stenosis close to the origin of the left renal artery (arrow). The stenosis was successfully treated with angioplasty and stenting.
Drugs
History
Patients with uncomplicated essential hypertension are asymptomatic and are identified only in the course of routine physical examination; however, patients with secondary hypertension may complain of symptoms from the underlying disorder.
[/not-level-membership-for-internal-medicine-category]
