[level-membership-for-basic-science-category]36
Hypercalcaemia




Diagnosis
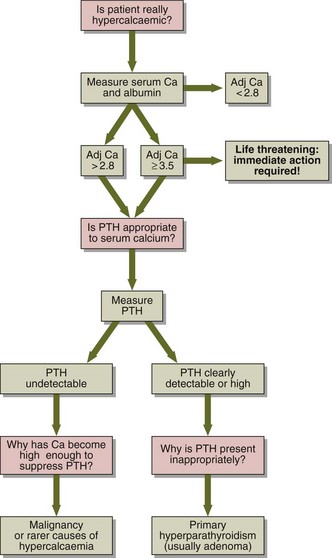
A diagnostic decision chart is shown in Figure 36.1. Primary hyperparathyroidism is most often due to a single parathyroid adenoma, which secretes PTH independently of feedback control by plasma calcium. Hypercalcaemia associated with malignancy is the commonest cause of a high calcium in a hospital population. Some tumours secrete a protein called PTHrP (parathyroid hormone-related protein), which has PTH-like properties.
Rarer causes of hypercalcaemia include:
 Inappropriate dosage of vitamin D or metabolites, e.g. in the treatment of hypoparathyroidism or renal disease or due to self-medication.
Inappropriate dosage of vitamin D or metabolites, e.g. in the treatment of hypoparathyroidism or renal disease or due to self-medication.

 Thyrotoxicosis very occasionally leads to increased bone turnover and hypercalcaemia.
Thyrotoxicosis very occasionally leads to increased bone turnover and hypercalcaemia.
 Thiazide therapy: the hypercalcaemia is usually mild.
Thiazide therapy: the hypercalcaemia is usually mild.
 Immobilization: especially in young people and patients with Paget’s disease.
Immobilization: especially in young people and patients with Paget’s disease.


 Diuretic phase of acute renal failure or in the recovery from severe rhabdomyolysis.
Diuretic phase of acute renal failure or in the recovery from severe rhabdomyolysis.

Treatment
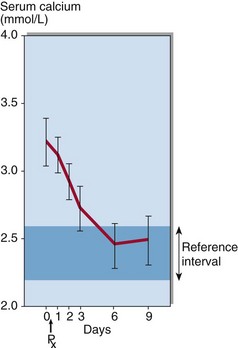
Treatment is urgent if the adjusted serum calcium is greater than 3.5 mmol/L; the priority is to reduce it to a safe level. Intravenous saline is administered first to restore the glomerular filtration rate and promote a diuresis. Although steroids, mithramycin, calcitonin and intravenous phosphate have been used, compounds known as the bisphosphonates have been found to have the best calcium-lowering effects. Bisphosphonates such as pamidronate have become the treatment of choice in patients with hypercalcaemia of malignancy (Fig 36.2). It acts by inhibiting bone resorption.
Familial hypocalciuric hypercalcaemia
Case history 29
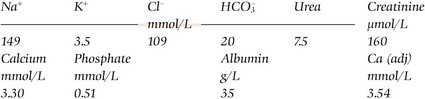
Biochemistry results in a serum specimen were:
 Clinical note
Clinical note
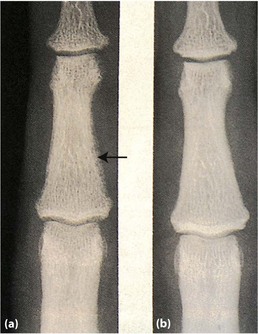
If hypercalcaemia is not detected early, the high circulating PTH causes a characteristic pattern of bone resorption, known as osteitis fibrosa cystica (shown in Figure 36.3). As awareness of hypercalcaemia has grown and detection methods have improved, such severe bone abnormalities are seen much less frequently.




[/level-membership-for-basic-science-category][not-level-membership-for-basic-science-category]36
Hypercalcaemia
Diagnosis
A diagnostic decision chart is shown in Figure 36.1. Primary hyperparathyroidism is most often due to a single parathyroid adenoma, which secretes PTH independently of feedback control by plasma calcium. Hypercalcaemia associated with malignancy is the commonest cause of a high calcium in a hospital population. Some tumours secrete a protein called PTHrP (parathyroid hormone-related protein), which has PTH-like properties.
Rarer causes of hypercalcaemia include:
Inappropriate dosage of vitamin D or metabolites, e.g. in the treatment of hypoparathyroidism or renal disease or due to self-medication.
Thyrotoxicosis very occasionally leads to increased bone turnover and hypercalcaemia.
Thiazide therapy: the hypercalcaemia is usually mild.
[/not-level-membership-for-basic-science-category]
