[level-membership-for-obstetrics-gynecology-category]CHAPTER 75
Hymenotomy (Hymenectomy)
Hymenectomy should be more accurately named partial hymenectomy, or hymenotomy. The operation is done primarily to diminish the discomfort of initial coitus in a virginal woman or to relieve dyspareunia for a woman already sexually active. The hymen is a point of constriction for intravaginal intercourse, and its stretching or tearing can be a significant source of discomfort during an ordinarily pleasurable physiologic act.
The patient is anesthetized, placed in the lithotomy position, prepared, and draped. The hymen is gently grasped with Adson-Brown forceps at the 1-o’clock position and with an Allis clamp at the 5-o’clock position. The hymen is placed on gentle traction with special care taken not to tear it by excessive force. A 1 : 100 vasopressin solution has been injected subdermally via a 27-gauge needle into the vestibule side just lateral to the hymenal attachment (Fig. 75–1A). The injection extends for the entire length of the hymen on the left side. The edge of the hymen is held with the Adson-Brown forceps and is placed on traction in the anterior direction. With the use of a scalpel (No. 15 blade), the hymen is cut free with a 2- to 3-mm margin from the vagina and vestibule, extending from the 1-o’clock position to just below 5 o’clock (Fig. 75–1B). The vagina is sutured with interrupted 3-0 Vicryl sutures to the vestibular margin (Fig. 75–1C). Next, Allis clamps are applied to the right side of the hymen at the 11-o’clock and 7-o’clock locations, and an identical procedure is performed. The operator’s two fingers are placed in the vagina to check for introital capacity. They should enter without resistance, and the introitus should accommodate them without significant counterpressure. It is preferred to leave intact the small area of hymen between the 5-o’clock and 7-o’clock positions and the remnant beneath the urethra. For reassurance, the patient is given vaginal forms to insert into the vagina after the 6-week postoperative check. A small or medium form is given to the patient initially. The form is well lubricated with a water-based personal lubricant (Astroglide) and is inserted into the vagina. The patient is asked to remove the form and insert it while the gynecologist views her technique. The patient is then instructed to insert it twice daily for 10 minutes (supine position) while relaxing her pelvic floor muscles around the form. Two weeks later, she is fitted with a large form (the size of an average erect penis). She continues her relaxation exercises. After 2 weeks, she can be assured that intercourse will take place normally and will be comfortable for her. Lubricant should be used with every sexual exposure for at least 30 days after initiation of regular intercourse (e.g., during and after the honeymoon).
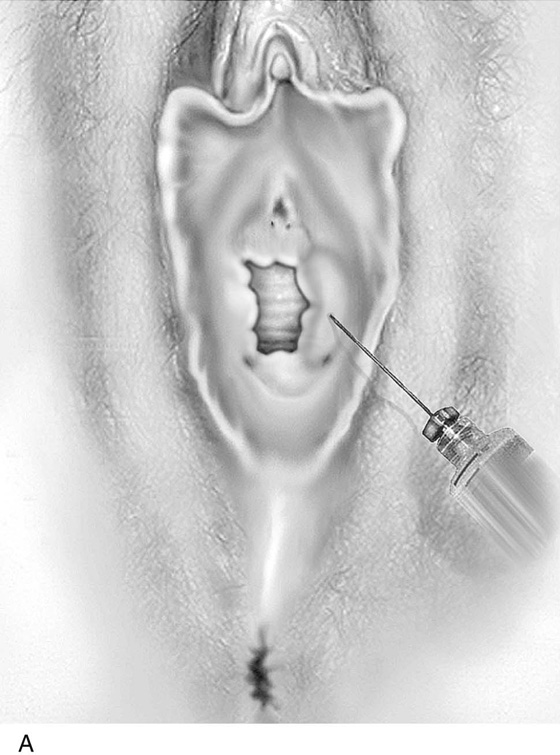
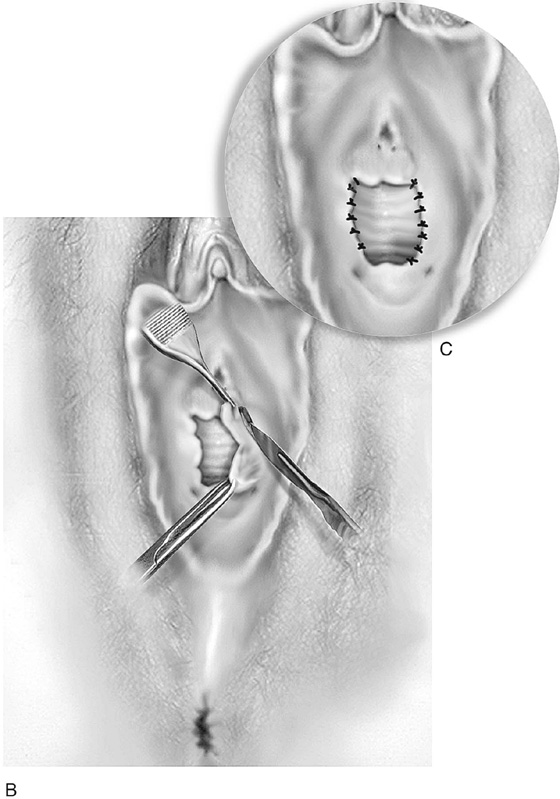
FIGURE 75–1 A. Initially, with a 10-mL syringe and a 1½-inch, 27-gauge needle, a 1 : 100 vasopressin solution (20 units/mL) is injected immediately lateral to the hymen, beginning at 5 o’clock and extending the needle subdermally to the 1-o’clock position. The solution balloons the surrounding vestibular and vaginal tissue. B. The hymen is grasped with Adson-Brown forceps at the 1-o’clock position. The lower portion of the hymen is held with an Allis clamp at the 5-o’clock position. The hymen is excised with a straight vertical knife cut, leaving a margin of vestibule (outer) and vagina (inner). C. The vaginal and vestibular margins are sutured together with interrupted 3-0 or 4-0 Vicryl sutures. An identical procedure is performed on the right side. The wound is irrigated with normal sterile saline and is observed to ensure that complete hemostasis has been obtained.
[/level-membership-for-obstetrics-gynecology-category][not-level-membership-for-obstetrics-gynecology-category]CHAPTER 75
Hymenotomy (Hymenectomy)
Hymenectomy should be more accurately named partial hymenectomy, or hymenotomy. The operation is done primarily to diminish the discomfort of initial coitus in a virginal woman or to relieve dyspareunia for a woman already sexually active. The hymen is a point of constriction for intravaginal intercourse, and its stretching or tearing can be a significant source of discomfort during an ordinarily pleasurable physiologic act.
The patient is anesthetized, placed in the lithotomy position, prepared, and draped. The hymen is gently grasped with Adson-Brown forceps at the 1-o’clock position and with an Allis clamp at the 5-o’clock position. The hymen is placed on gentle traction with special care taken not to tear it by excessive force. A 1 : 100 vasopressin solution has been injected subdermally via a 27-gauge needle into the vestibule side just lateral to the hymenal attachment (Fig. 75–1A
[/not-level-membership-for-obstetrics-gynecology-category]
