Chapter 24 Hunting and Fishing Injuries
For online-only figures, please go to www.expertconsult.com 
Hominids were at a disadvantage, even in groups, when hunting large animals or driving off other predators from their kills until they began using stones, long bones, and sticks to enhance their relatively weak teeth and claws. Implements for hunting and skinning animals were the earliest tools found by anthropologists. Human cultural evolution followed closely the technologic changes in weapons, although sports, business, and war had replaced the need for hunting in most cultures, even by the time Nimrod walked the earth. Bows and arrows, slings, spear throwers, nets, harpoons, traps, and firearms were designed to extend the reach and increase the lethality of the human hand. Unfortunately, humans discovered that they could kill each other with these weapons. Since the discovery of gunpowder, the development of weapons technology has surpassed all other forms of human endeavor, including medicine and transportation.4,5,14
Hunting in the United States
The North American Association of Hunter Safety Coordinators (NAAHSC), a division of the New York State Office of Wildlife Management, reported 860 fatal hunting injuries in the United States during the 4-year period between 1983 and 1986, with a total of 6992 injuries from firearms.44 Interestingly, 34% of the total injuries and 89% of the handgun injuries were self-inflicted. Shotguns accounted for 106 of the fatalities and 906 of the total injuries, whereas rifles accounted for 79 fatalities and 465 injuries. The New York State Department of Environmental Conservation reported that the average number of hunting injuries decreased from an average of 137 per year in the decade of the 1960s to only 48 in 2001 and 37 in 2002.8 They credit the institution of hunter safety programs in 1960. In 2001 Colorado reported 9 injuries and 1 death per 500,000 licensed hunters.11 Michigan reported 2 deaths per 2,665,952 hunters in 2003, giving hunting one of the lowest injury and fatality rates of any recreational activity.57
The type of hunting also influences the rate of injury. Smith and colleagues51 reviewed 1345 hunting injuries in Pennsylvania from 1987 to 1999. They showed that turkey hunters had the highest rate of injury (7.5 per 100,000 hunters) and grouse hunters the lowest (1.9 per 100,000 hunters). This was attributed to turkey hunters not wearing orange hunter clothing. Deer hunters had the highest case-fatality ratio at 10.3%, and pheasant hunters the lowest at 1.3%. This higher fatality rate was largely because most deer-hunting injuries were due to wounds caused by rifle bullets. They also noted that younger hunters suffered the highest rate of injuries, and the largest percentage of incidents occurred on opening day.
Hunting-related shootings represent a very small portion of the total number of accidental firearm deaths in the United States. In Colorado, from 1997 to 2005, there were four deaths during hunting, all attributed to cardiac causes, and none in hunters from firearms, falls, or penetrating injuries. The most common traumatic injuries were lacerations; 75% of lacerations were from knife injuries while field dressing the animals. Of 131 unintentional firearm deaths in California from 1977 to 1983, only 8 were the result of hunting accidents.*
Types of Injuries Encountered
Blowguns, although mainly used by aboriginal hunters, have become popular with some recreational hunters of birds and small game. The blowgun varies in length, and a variety of darts can be projected 6 to 15 m (19.7 to 49.2 feet) by the exhaled breath. The darts have low energy and do not penetrate very deeply. Modern blowguns rarely cause serious injury unless striking the eye or possibly a blood vessel. To effectively kill small game, the darts generally must carry an immobilizing or poisonous toxin. Darts used by some tribes contain toxins derived from both animal and plant sources. These toxins can cause paralysis and death in humans who have been punctured by the dart either accidently during transport or purposefully during tribal war. Animal toxins are primarily neuromuscular toxins and many have been developed for medical use. South American tribes have used Dendrobates frog toxins, which are steroidal alkaloid compounds known as batrachotoxins and homobatrachotoxins. These toxins act at voltage-gated sodium channels and cause irreversible depolarization of nerves and muscles. Several other toxins, including gephyrotoxin, pumiliotoxins, histrionicotoxins, and epibatidine, have been isolated from poison dart frogs. The last toxin is the most potent nicotinic agonist known and is a powerful nonopiate analgesic. Interestingly, these frogs lose their ability to produce toxins in captivity, leading to the finding that the frog’s diet of Melyridae beetles actually is the source of the toxins. Plant-derived toxins include strychnine, curare, and a number of cardiac glycosides from Africa, South America, and Asia, where dart and arrow poisons are still used by indigenous people. All of these toxins, especially the cardenolides from the Maquira, Naucleopsis and other Moraceae species, have been studied for possible medicinal value.46,49
Veterinarians commonly use air-powered darts fired from rifles or blowguns to subdue large animals. These darts contain pharmacoactive agents, such as succinylcholine, phencyclidine, ketamine, and xylazine, in concentrations great enough to bring down an elephant, lion, or rhinoceros. The darts are 3-mL plastic syringes with 16-gauge needles delivered using a 1.8-m (5.9-foot) blowgun or rifle. Accidental human injection can be rapidly fatal if reversing agents or advanced life support is not available. Homemade blowguns are frequently used for sport and usually consist of a needle or pin attached to a wooden shaft and a cotton ball or piece of yarn for a feather. Although these darts do not contain any toxins, they are still capable of causing injuries, especially to the eye. There have been reported cases of aspiration of darts.27,29,59
Tree Stand Injuries
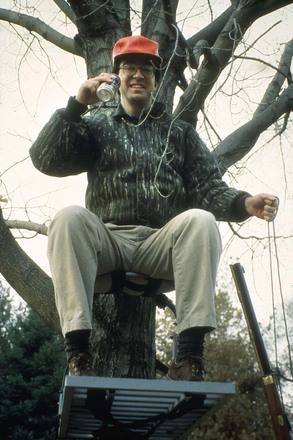
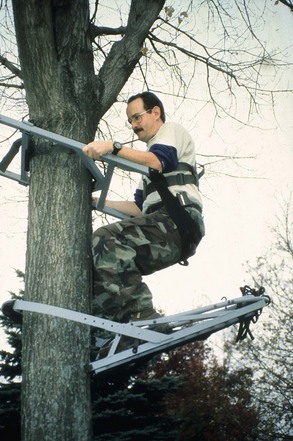
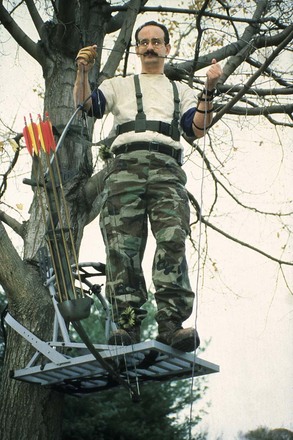
A frequent preventable cause of serious injury and death among hunters is not associated with firearms at all. It is the tree stand injury. Tree stands are small platforms designed to hold hunters high above the ground so they can more easily spot and kill large game while remaining undetected. Whether homemade or of commercial design, the platforms generally are small, portable devices that the hunter attaches to the trunk of a tree near game trails or water holes. The stands may have attached ropes or ladders for access, or the hunter may free-climb the tree for placement of the stand or fasten small climbing steps on the tree (Figures 24-1 and 24-2). Hunters may fall asleep on the platforms and fall off or fall while climbing up or down trees. At least one-half of these injuries could be prevented if all hunters wore tree stand safety harnesses (Figure 24-3). Although most of the injuries are similar to those seen with any type of fall, occasionally a hunter drops a firearm, which discharges, or falls on an arrow or rifle, causing an additional weapons injury. Over 10 years, injuries of this type in Georgia accounted for 36% of reported hunting injuries and 20% of hunting fatalities.7 A study from the University of Rochester, New York, looked at tree stand injuries from 1996 to 2001.47 The authors noted that 51 injuries occurred, all in men, with a mean age of 42. Alcohol was present in 10% of patients and 2 of 3 deaths. Spinal fractures were the most common injuries (51%), followed by extremity (41%), head (24%), and lung injuries (22%). Only two patients had been using a safety belt (4%). Sixteen spinal cord injuries were reported between 1987 and 1999 in Oklahoma; the mean height of fall was 16 feet, and 18% were related to alcohol ingestion. Ninety percent resulted in paraplegia/paraparesis, and 12.5% were fatal.*
Arrow Injuries
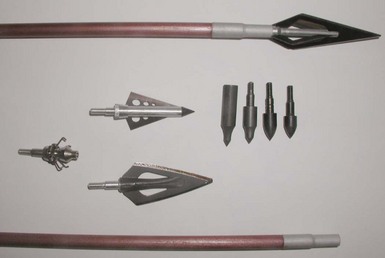
Modern arrows are usually made from aluminum, graphite, or fiberglass, although many beginners still use inexpensive wooden arrows. A number of types of arrowhead are in use, such as field points and target points, but most injuries are due to specially designed hunting arrowheads called broadheads. These razor-sharp metal points come in a variety of sizes and shapes and are designed to kill game by lacerating tissue and blood vessels, causing bleeding and shock. Unlike hunting firearms projectiles, which are designed to kill quickly through massive tissue damage and rapid incapacitating hemorrhage, arrows usually kill more slowly with less tissue damage (Figure 24-4).3,22,23,25Arrows are propelled by a conventional bow, which may be straight, recurved, or compound, or by a crossbow. Crossbow projectiles may be called arrows or bolts and generally are shorter and heavier than arrows fired from a bow. The force used to propel the arrow is usually measured in draw weight, which is the number of foot-pounds necessary to draw a 71.1-cm (28-inch) arrow to its full length. The higher the pound draw, the more powerful the bow and the deeper the penetration acheived by the same type of arrow.
Injuries From Firearms
Nonpowder Firearms
Whereas traditional firearms discharge a projectile by the contained expanding gases generated in the gun barrel by modern fast-burning powders or old-fashioned black powder, nonpowder firearms use a spring, compressed air, or carbon dioxide cartridge to accelerate the projectile out of the barrel. Although air guns are quite accurate at short distances and can develop muzzle velocities in excess of 365.8 m/sec (1200 ft/sec), the small lightweight projectiles usually cannot penetrate skin at distances greater than 100 m (328 feet). Nonpowder firearms are commonly used by children, who cannot legally obtain or use other types of firearms. Uninformed parents buy them as toys, erroneously believing them to be harmless by design. Without supervision and proper training in gun safety, severe injury and death can result. The wounds they cause can be lethal, especially from high-powered air rifles, which can send out pointed projectiles at sufficiently high velocities to penetrate the skull and body cavities. In a recent technical report, Laraque and colleagues estimated 21,840 injuries during the year 2000 from nonpowder firearms, with a 4% hospitalization rate. There were 39 resultant deaths between 1990 and 2000. Care must be taken not to trivialize these injuries, especially in the pediatric patient, where softer, thinner bone may lead to deep penetration by even lightweight projectiles.* Less than lethal (LTL) rounds are used by police and military to subdue individuals without causing serious injury. These rounds may be rubber, wooden, synthetic sponge, or soft wax. Although designed to disperse a crowd or incapacitate a person until he or she can be subdued, they can cause significant injury. This usually occurs when the person is struck in the head or in some cases the abdomen or thorax. These rounds are not designed for hunting but may be encountered if used by the uninitiated. Rounds such as airsoft are used in many police and military training facilities to add realism to the training scenario. These rounds may cause eye injuries if safety precautions are not used.21,31 Paintball guns, although not designed or generally used for hunting, are commonly used in outdoor activities that mimic tactical games. Most injuries occur in children who are not wearing eye protection, but there are also reported cases of vascular injuries. Paintballs are 14-mm (0.6-inch) gelatin capsules that are filled with water-soluble paint of various colors. Because of their small size, they can bypass the bony orbital protection of the eye. Paintballs propelled by carbon dioxide can travel over 91.4 m/sec (300 ft/sec). At this velocity, the globe, cornea, and retina can be disrupted with a direct hit. The American Society for Testing and Materials has standards for eye protection for paintball sports. These include a helmet with integral eye, face, and ear protection (Figure 24-5). Unfortunately, many children either do not wear the recommended protection or remove it during play because of fogging or discomfort.12,24,28,30,38

Powder Firearms
Black powder weapons use a centuries-old slow-burning propellant that is ignited with a spark from flint striking steel or a percussion cap. The firearms are usually single shot and loaded from the muzzle by pouring a measured amount of black powder down the barrel and then inserting the projectile and tamping it down onto the powder charge. When ignited, the propellant is converted to a gas that expands and pushes the projectile out of the barrel of the weapon. With modern design and manufacturing techniques, these weapons are sufficiently accurate to hunt large game, such as deer and elk. The injuries from black powder weapons are similar to those from modern weapons and are discussed later. The same precautions should be used when hunting with or shooting any type of firearm, whether the propellant is air or gunpowder.1,2,13,45
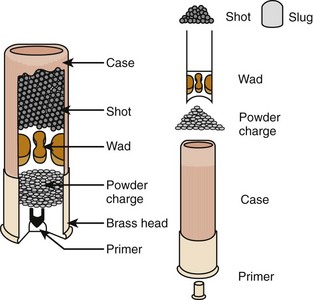
The term cartridge is used to refer to the intact, unfired assembly of projectile and propellant loaded into the gun for firing. Rifle and pistol cartridges consist of a metal case that contains the gunpowder propellant and into which the bullet is seated and held by compressing the case around the bullet base at the time of manufacture. The base of the case contains a small metal primer filled with a small amount of high explosive that serves to ignite the fast-burning propellant when it is struck by the firing pin of the gun. The primer is in the center of the base of the case (center-fire ammunition) in all cartridges except in small-caliber .22 cartridges, where it is incorporated into the entire circumference of the cartridge base rim (known as rimfire ammunition). Rifle and pistol cartridges generally contain a single bullet, although some may be loaded with very small shot to increase the probability of hitting small objects at short distances. Shotgun cartridges consist of a center-fire metal base combined with a paper or plastic shell in the form of a closed-end tube. Within this tube is placed the propellant and then the projectile(s), along with associated plastic, cotton, or paper materials collectively referred to as wadding (Figure 24-6).
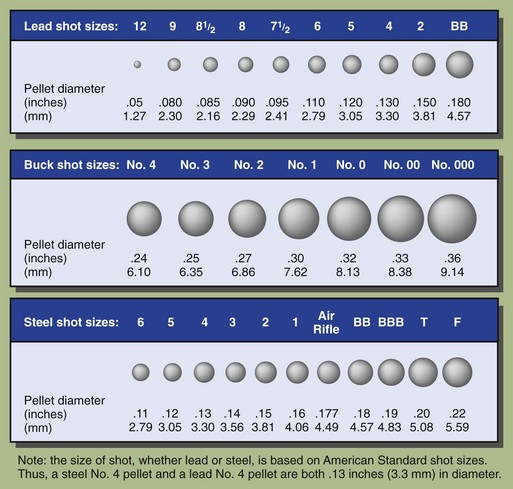
Shotgun projectiles consist of shot ranging in size from 1 to 10 mm (0.04 to 0.4 inch) (Figure 24-7) or a single solid projectile known as a slug. Shot pellets used to be made of lead. Because of high lead levels in ducks and geese that ingested spent shot while feeding, lead shot for bird hunting was banned in 1991. Approved shot may be made of steel, tin, or various mixtures of tin, bismuth, and up to 15% iron. Steel shot can be identified on radiographs because it retains a perfect round shape, whereas lead and tin shot deforms inside the barrel during firing, resulting in nonspherical shapes. Determining the shot type can help clinicians decide about the safety and usefulness of magnetic resonance imaging scans in the setting of steel projectiles, or the risk for lead toxicity.
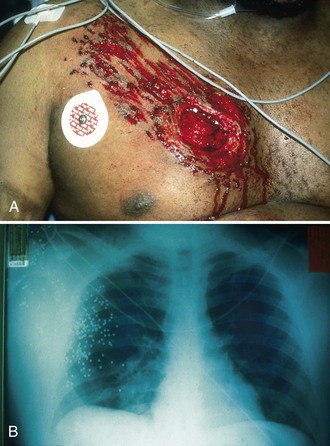
Beside the wadding and projectile(s), hot gas and unburned powder also exit the muzzle. In cases of close-proximity wounds, usually under 1.1 m (3.5 feet), powder stippling may appear on clothing or skin. The presence of powder stippling or wadding in a wound may have important forensic applications and should always be noted. With contact wounds, where the muzzle is pressed into the skin at the time of firing, escaping hot gases may enter the wound channel and expand inside the victim, causing burns, organ damage, burst skin, and/or a stellate laceration around the point of entrance. Figures 24-8 to 24-10 show examples of gunshot wounds.


FIGURE 24-9 Shotgun wound to the upper arm. Initially the wound looked benign. Both entrance and exit can be seen.
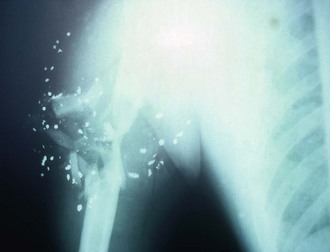
FIGURE 24-10 Radiograph of the same shotgun wound to the upper arm as seen in Figure 24-9. Extensive bone and soft tissue injury, as well as vascular and nerve damage, can be seen.
Magnum refers more to the type and amount of powder than to the size of the bullet used. Magnum cartridges are designed to give hunters the ability to successfully hunt large game with pistols by improving terminal ballistic performance of the bullet. Figure 24-11 shows some examples of different bullets. Shotgun terminology is a little less complicated, based on the number of lead balls, the diameter of the barrel, and how many lead balls it takes to make a pound. For example, a 12-gauge shotgun has a barrel that is the same diameter as a lead ball that weighs 0.08 lb (37.6 g); a 20-gauge, 0.05 lb (22.7 g). The higher the gauge number, the smaller the barrel and the smaller the projectile. The only exception is the .410 shotgun, which is caliber .410, or 0.410 inch (1 cm) in diameter. Figure 24-12 shows some examples of shotgun rounds and the shot and wadding within them.


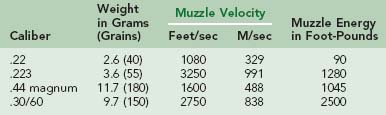
The type and severity of wounds inflicted by a firearm depend on several factors. The most often quoted factor, but the least important, is the amount of energy the bullet (projectile) has when leaving the firearm. The kinetic energy formula, Ek =  MV2, can be applied to any moving object and can be used to calculate the muzzle energy for a particular type of firearm. Energy increases much more as a function of the velocity of the bullet than as a function of the mass. For this reason, most firearms are classified according to muzzle velocity. The higher the velocity of the bullet, the greater the energy and the greater the potential for injury. Firearms with muzzle velocities greater than 762 m/sec (2500 ft/sec) are considered high velocity, 457.2 to 762 m/sec (1500 to 2500 ft/sec) are medium velocity, and less than 457.2 m/sec (1500 ft/sec) are low velocity (Table 24-1).
MV2, can be applied to any moving object and can be used to calculate the muzzle energy for a particular type of firearm. Energy increases much more as a function of the velocity of the bullet than as a function of the mass. For this reason, most firearms are classified according to muzzle velocity. The higher the velocity of the bullet, the greater the energy and the greater the potential for injury. Firearms with muzzle velocities greater than 762 m/sec (2500 ft/sec) are considered high velocity, 457.2 to 762 m/sec (1500 to 2500 ft/sec) are medium velocity, and less than 457.2 m/sec (1500 ft/sec) are low velocity (Table 24-1).
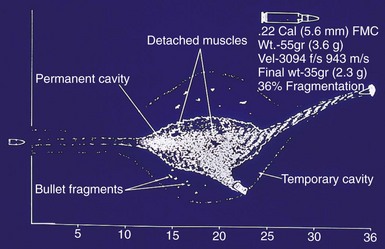
Bullets cause damage to tissue by crushing. The energy of a bullet may be transmitted to the tissue in part or in total depending on the surface area the bullet presents to the tissue. Bullets that yaw, expand, or fragment present more surface area than do bullets that stay in one axis and maintain one shape. By international agreement codified in the articles of the Hague Convention IV of 1907, military bullets are not to be designed in a manner to produce “superfluous” wounding effects by features that would encourage the bullets to flatten or expand on impact with tissue. They are typically completely encased in a copper jacket to prevent deformation of the soft lead core. Such rounds generally pass through an individual, leaving a permanent wound tract similar in diameter to that of the bullet. The ammunition is designed to wound a soldier and put him or her out of combat, but not to kill the soldier. In contrast, hunting ammunition is designed to expand on impact up to two or three times its diameter, resulting in a much larger wound channel, greater tissue damage, and rapid incapacitation and death (Figure 24-13). This feature of planned deformation also promotes retention of the bullet within the target and reduces the risk for injury to unseen individuals downrange from the game animal. In fact, many states require the use of expanding ammunition for hunting large game. This may increase the wound severity of hunting injuries compared with military and criminal shootings.

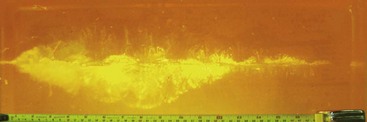
To allow laboratory comparison of projectile designs and to study the effect of velocity and expansion, experimental wounding profiles have been described using ballistic gelatin, which accurately simulates human muscle tissue. These wounding profiles show the various aspects of potential ballistic injury, including cavitation, yaw, and fragmentation (Figures 24-14 and 24-15).19 The total effect of high energy, fragmentation, expansion, yaw, and temporary cavity formation results in tissue injury. Although the kinetic energy formula yields the total energy available to cause injury, the physical behavior of the projectile(s) and the transited tissues are the actual determinants of the complete injury pattern. The type of tissue struck is the most important factor. As can be seen from Table 24-1, the .22-caliber long rifle rimfire bullet has a low mass and velocity and thus a low muzzle energy, yet more fatalities have occurred from this round than from any other. It is very inexpensive, can be fired from a number of rifles and handguns, is commonly used to hunt game, and is not thought of as particularly dangerous by inexperienced hunters. For these reasons, more people are shot by this cartridge than by any other single bullet type. The bullet is highly lethal when striking the brain, heart, or a major blood vessel.* Rubber or plastic bullets, although generally not used for hunting, may be encountered. These bullets travel at about 61 m/sec (200 feet/sec) and will not usually penetrate skin, although at short ranges (under 15.2 m [50 feet]) they can cause fractures, eye trauma, and other blunt injuries.19
Trap Injuries
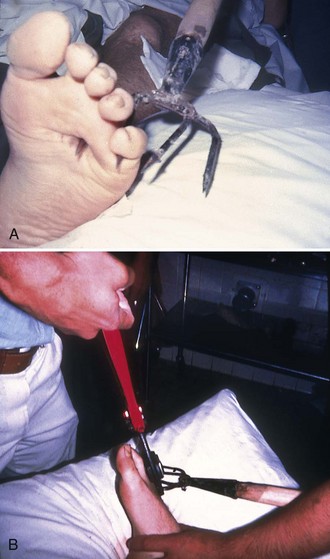
Traps are designed either to kill animals or to capture them alive and uninjured. The latter type poses no risk to humans unless they should happen upon a trap and attempt to free the animal or otherwise approach the trap. The trapped animal often will bite or claw anyone within range. Leghold traps designed to kill or injure an animal may occasionally cause problems for unwary hikers or campers. These traps have a spring-loaded jaw that closes when triggered by something touching the trigger plate, usually involving only 0.5 to 1 kg (1 to 2 lb) of pressure. Most injuries involve the foot, but any area of the body that can fit between the jaws potentially can be injured. The jaws can be released by compressing the spring controlling the jaws (Figure 24-16). Very large traps used to trap poachers or to catch large animals, such as tigers or bears, cannot easily be released without help. These traps may also be attached to large weights, such as logs or concrete blocks, to prevent escape. Fortunately, most of these large traps are now collector’s items and not used in the field.

Many injuries occur when the person setting the trap inadvertently causes the trap to spring before being set in the ground. This often causes hand and finger injuries, especially with amateur trappers unfamiliar with the type of trap (Figure 24-17). Unconventional traps, such as snares, deadfalls, and pit traps, may rarely be encountered, but the mechanisms and types of injuries are quite variable. Trap guns are illegal in most areas of the world; injuries are similar to gunshot wounds.

Treatment of Hunting Injuries
Arrow Injuries
Lacerations from razor-sharp hunting points are not unusual and can be treated like any similar laceration. The wound should be irrigated, any foreign material removed, and the laceration closed primarily. Victims pierced by an arrow should be stabilized, and the arrow should be left in place during transport, if possible. Attempts to remove the arrow by pulling it out or pushing it through the wound may cause significantly more injury and should be avoided. It is acceptable to cut off the shaft of the arrow and leave 8 to 10 cm (3 to 4 inches) protruding from the wound to make transport easier if this can be accomplished with a minimum of arrow movement. A large pair of paramedic-type shears can usually cut through an arrow shaft if it is stabilized during cutting. The portion of the arrow that remains in the wound should be fixed with gauze pads or cloth and tape. A similar approach should be used for spears and knives. The victim should be transferred as quickly as possible to an operating room, where the arrow can be removed under controlled conditions. Radiographs are helpful to identify associated anatomic structures before removal is attempted in the operating room (Figure 24-18).

Gunshot Wounds
Myths About Gunshot Wounds
Many myths associated with the management of gunshot wounds should be repudiated.
Emergency Department Care
Victims in shock should be taken to the operating room immediately to control bleeding. If this is not possible, type O-negative or type-specific blood should be transfused. Autotransfusion, when available, can be an ideal way to replace lost blood in the victim in shock. Starch or other blood substitutes may raise the blood pressure temporarily, but large amounts of crystalloid fluids may cause increased bleeding. Hypotensive resuscitation, which allows the patient to remain relatively hypotensive as long as organ perfusion is adequate, may be the best intervention if an operating room is not readily available. A systolic blood pressure of 80 mm Hg may not be “normal,” but it may be sufficient for a supine patient. Increasing the blood pressure to 110 mm Hg may seem “normal,” but it may also cause rebleeding and irreversible shock. Hypotensive resuscitation should be the standard unless the patient loses his or her pulse or level of consciousness. At that time, blood products are the fluids of choice, followed by a starch such as hetastarch (Hextend). Level of consciousness and return of pulse should be the clinical goals. Once the bleeding is controlled, fluid resuscitation based on physiologic criteria, such as blood pressure, hematocrit, oxygenation, and acid-base status, can be used. Military antishock trousers or pneumatic antishock garments have not been shown to be beneficial in the treatment of shock secondary to penetrating trauma. Emergency thoracotomy is indicated for victims who have lost vital signs shortly before reaching the emergency department or while in the emergency department. Injuries to the heart or great vessels can be occluded with Foley catheter balloons, pericardial tamponade can be relieved, and the aorta can be cross-clamped. Hypothermia is commonly unrecognized in the trauma victim and may lead to coagulopathy, cardiac arrhythmias, or electrolyte disturbances. Rectal temperatures should be obtained and only warmed fluids and blood given to the victim.13,26,33,60
Wounds from high-velocity bullets are similar to other types of wounds, and standard rules of debridement should be followed. Wide debridement of normal-appearing tissue is unnecessary and should not be done. In general, victims of gunshot wounds should be evacuated quickly and stabilized if possible. Most victims (80%) of gunshot wounds to the chest who survive the first 30 minutes can be treated with a thoracostomy tube and observation.33 The amount of blood that is drained from the thoracostomy tube determines whether operative intervention is necessary. Draining more than 1500 mL of blood immediately or more than 200 mL/hr for over 4 hours is an indication for thoracotomy. Signs of pericardial tamponade are an indication for immediate pericardiocentesis and operative repair. All gunshot wounds to the abdomen should be explored in the operating room. These include all penetrating injuries below the nipples and above the symphysis pubis.
Vascular injuries may not be identified during the initial examination; therefore noninvasive, portable, Doppler ultrasound studies can be extremely valuable in the emergency department. Contrast angiography should be performed on any victim with a suspected vascular injury. The removal of the bullet or bullet fragment is not necessary unless the bullet is intravascular, intra-articular, or in contact with nervous tissue, such as the spinal cord or a peripheral nerve. Bullets found during exploratory laparotomy or wound debridement should be removed, but it is unnecessary to explore soft tissue, such as muscle or fat, solely to remove a bullet. Shotgun pellets that have minimal penetration can be removed from the skin with a forceps. Plastic or cloth wadding found in superficial shotgun wounds should be removed. Shotgun blasts may produce large soft tissue defects that need extensive debridement and either skin grafting or surgical flap rotation to maximize coverage. Patients with powder burns should have as much of the powder residue removed as possible with a brush under local anesthesia. The powder will tattoo the skin if it is not removed, and the deep burns may need dermabrasion or surgical debridement (Figure 24-19).13,60,61,63
Retained lead bullets and shotgun pellets for the most part are not hazardous; however, when they are within joint spaces or the gastrointestinal tract, significant amounts of lead can be absorbed and toxicity can occur. Infection of gunshot wounds is common, especially with large tissue injuries, injuries to the bowel and wounds that are highly contaminated with clothing or other debris. Despite myths to the contrary, bullets are not sterile. Certainly, clothing, skin, and other substances that the bullet may acquire during flight are not sterile.52
Prevention of Hunting Injuries
Most injuries could probably be prevented by following a few simple rules. Nonhunters should be aware of hunting seasons and designated hunting areas and wear international orange clothing while in hunting areas (Figure 24-20). Hunters should always be sure of their target before shooting, use safety harnesses in tree stands, and use appropriate technique and tools for cleaning game. Tree stands should be well constructed. Hunters should never consume alcohol or mind-altering drugs that might interfere with their judgment. Eye protection in the form of safety glasses should be worn while hunting or target shooting to prevent injuries from ricocheting fragments and shotgun pellets. High-frequency hearing loss is common in hunters because of the loud report of the firearm. Although earplugs and headsets can protect the hunter, they are impractical for most hunting and are used mainly for target shooting. Some hunters use a single ear plug for the ear closest to the muzzle of the firearm. This protects the ear most likely to be injured but still allows the hunter to hear approaching game and other hunters. Bow hunters should always use wrist and finger protection to prevent injuries from the arrow fletching and the bowstring. All arrows should be carried in a quiver until ready for use. The broadhead arrow should always be pointed away from the hunter. These few steps would probably eliminate most hunting injuries.45,47

Fishing Injuries
Fishhook Injuries
Fishhooks can penetrate skin, muscle, and bone, and they may pierce the eye or the penis. Care must be taken in removing a fishhook so that further damage to underlying structures is avoided. The first step is to remove the portion of the hook that is embedded from any attached lines, fish, bait, or lure. This is best done with a sharp side-cutting pliers. A bolt cutter may be needed for large, hardened hooks such as used in shark or swordfish fishing. Treble hooks, with three separate hooks attached at a single eye, are designed to improve the chance of catching a fish going after a live or artificial bait (Figure 24-21). They are also used in “snagging” fish, in which the line with one or more treble hooks is pulled through the water in an attempt to snag a fish on any part of its body. They may be found on many types of fishing lures, some with three or more treble hooks on a single lure (Figure 24-22, online). When this type of hook is embedded, often more than one of the hooks is involved. Cutting the embedded hooks off the lure or the treble hook will prevent further injury before removal. Most fishermen carry a multitool or needle-nose pliers for removing hooks and lures from fish. These same tools can be used in the field to remove or stabilize embedded hooks.


A number of techniques are used for removing embedded fishhooks, but all involve a certain amount of movement of the hook, which causes increased pain. A local anesthetic should be infiltrated around the puncture site to minimize pain and movement of the patient. The following method can be used if the hook is not deeply embedded (Figure 24-23, E ). Pressure is applied along the curve of the hook while the hook is pulled with a snapping motion away from the point. Because the barb is on the inside of the curve of the hook, this enlarges the entrance hole enough to allow the barb and point to pass through. Sometimes a string looped through the curve of the hook facilitates the process. If the hook is deeply embedded, pressure can be applied along the curve of the hook to advance it further into the tissue until the point and barb penetrate the skin at another place on the surface, and then the barb can be cut off and the remainder (shaft) of the hook backed out (Figure 24-23, A to D).
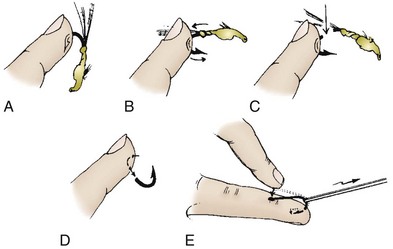
FIGURE 24-23 A to D, Removal of a fishhook that has deeply penetrated a fingertip. E, “Press-and-yank” method of fishhook removal.
Most fishhook injuries are not significant. However, penetrating eye injuries can lead to loss of vision in one or both eyes. These type of injuries can occur when the angler has snagged the fishing lure on a rock or other object and in order to attempt to free the lure, gives a pull that displaces the lure and strikes the angler in the eye. This can also occur when attempting to land a fish, when the lure pulls out of the fish’s mouth and strikes the angler in the eye. Many anglers also hook other anglers stationed behind them in a boat or on shore with their backcast. Fishhooks embedded in the eye should be left in place; the eye covered with a noncompressing metal patch, goggles, glasses, or cup; and the victim referred to an ophthalmologist for further care. Local anesthetic can be used to anesthetize the eye before applying the protection. If possible, the body of the fishing lure should be separated from the hook if it can be done without causing further harm. A wire cutter or multipurpose tool can be used for this (Figure 24-24). A plastic cup can be cut to size, or safety glasses or goggles can be used as an expedient eye shield. A pressure patch should not be applied, because this may lead to more serous injury. The cup, glasses, or goggles should be taped in place to prevent the victim from touching the eye and to prevent displacement during evacuation. It is not necessary to patch both eyes (Figures 24-25 to 24-27). All persons with penetrating eye injuries should be given oral antibiotics as soon as possible to prevent vision-threatening endophthalmitis. Rarely hooks become embedded in bone or cartilage; this victim must be taken to the operating room to have the hook removed via a surgical incision.




Fishing Spear Injuries
Fishing spears, like fishhooks, are designed to penetrate and hold fish. They may be jabbed, thrown, or propelled by rubber straps or carbon dioxide cartridges. The more force used to propel the spear, the deeper the penetration into tissue. Although arrows are designed to cause bleeding and bullets to cause crushing, fishing spears are designed to hold the fish until it drowns or is otherwise dispatched. Spears may penetrate the human chest or abdominal cavity, skull, or any other anatomic area. Some bleeding may occur, especially if major blood vessels are struck. The victim should be removed from the water as soon as possible and immediate attention given to airway, breathing, and bleeding control. The spear should be stabilized in place, and the victim immediately transported to a medical facility. Penetrating neck and chest injuries may require endotracheal intubation and tube thoracostomy. If a spear is embedded in the victim’s cheek and interferes with his or her airway, cutting the spear off with a bolt cutter and removing it through the mouth is permitted. Spears in all other locations should be left in place, although they may be cut off to facilitate transportation or improve the victim’s comfort (Figure 24-28).41
Other Fishing Injuries
Although spears and hooks cause the majority of penetrating injuries, fishing weights or sinkers can also be hazardous. Fishing sinkers are usually composed of lead and range in size from a few grams to 85 to 113 g (3 to 4 oz). When propelled by the action of a rod, they may act as projectiles with quite a bit of kinetic energy. Ancient hunters and warriors used lead and stone projectiles propelled by slings to hunt game or in battle to inflict serious injuries. The energy stored in a 2.1-m (7-foot) fiberglass fishing rod is potentially more than that delivered by a standard sling, so it is not surprising that an injury such as the one shown in Figure 24-29 is possible.

1 Adams DB. Wound ballistics: A review. Mil Med. 1982;147:831.
2 Amato JJ, Syracuse D, Seaver PRJr, et al. Bone as a secondary missile: An experimental study in the fragmentation of bone by high-velocity missiles. J Trauma. 1989;29:609.
3 Bear F. Fred Bear’s world of archery. Garden City, NY: Doubleday; 1979.
4 Blumenschine RJ, Cavallo JA. Scavenging and human evolution. Sci Am. 1992;267:90.
5 Campbell BG. Hunting and the evolution of society. In: Humankind emerging. Boston, Little: Brown; 1979.
6 Carter GL. Accidental firearm fatalities and injuries among recreational hunters. Ann Emerg Med. 1989;18:406.
7 Centers for Disease Control and Prevention. Tree stand-related injuries among deer hunters—Georgia, 1979-1989. MMWR Morb Mortal Wkly Rep. 1989;38:697.
8 Centers for Disease Control and Prevention. Hunting-associated injuries and wearing “hunter” orange clothing, New York 1989-1995. MMWR Morb Mortal Wkly Rep. 1996;45:884.
9 Christensen TL, Brandes SB. Urologic injuries sustained after free falls from hunting tree stands. South Med J. 2008;101:383.
10 Cole TB, Patetta MJ. Hunting firearm injuries, North Carolina. Am J Public Health. 1988;78:1585.
11 Colorado Division of Wildlife. Annual law enforcement and violation report. Denver: Colorado Division of Wildlife; 2001.
12 Conn JM, Annest JL, Gilchrist J, et al. Injuries from paintball game related activities in the United States 1997-2001. Inj Prev. 2004;10:139.
13 Department of Defense. Emergency war surgery, rev 3. Washington, DC: I. Borden Institute; 2004.
14 Dupuy TN. The evolution of weapons and warfare. New York: Bobbs-Merrill Co; 1980.
15 Fackler ML. Wound ballistics: A review of common misconceptions. JAMA. 1988;259:2730.
16 Fackler ML, Bellamy RF, Malinowski JA. Wounding mechanism of projectiles striking at more than 1.5 km/sec. J Trauma. 1986;26:250.
17 Fackler ML, Bellamy RF, Malinowski JA. The wound profile: Illustration of the missile-tissue interaction. J Trauma. 1988;28:S21.
18 Fackler ML, Malinowski JA. The wound profile: A visual method for quantifying gunshot wound components. J Trauma. 1985;25:522.
19 Fackler ML, Surinchak JS, Malinowski JA, et al. Bullet fragmentation: A major cause of tissue disruption. J Trauma. 1984;24:35.
20 Fayssoux RS, Tally W, Sanfilippo JA, et al. Spinal injuries after falls from hunting tree stands. Spine J. 2008;8:522.
21 Feier CC, Mallon W. Injury pattern of the stingball. J Emerg Med. 2010;38:444.
22 Geissinger G, Magid GA, McMahon RC. Arrow trauma to cervical spine. Wis Med J. 2009;108:197.
23 Grellner W, Buhmann D, Giese A, et al. Fatal and non-fatal injuries caused by crossbows. Forensic Sci Int. 2004;142:17.
24 Guerrero MA, Zhou W, El Sayed HF, et al. Subcapsular hematoma of the kidney secondary to paintball pellet injuries. J Emerg Med. 2009;36:300.
25 Hain WH. Fatal arrow wounds. J Forensic Sci. 1988;34:691.
26 Halanski MA, Corden TE. Wisconsin firearm deer hunting season: Injuries at a level 1 trauma center, 1999-2004. Wis Med J. 2008;107:2024.
27 Herbst LH, Pacher C, Seal US. Immobilization of free-ranging African lions (Panthera leo) with a combination of xylazine hydrochloride and ketamine hydrochloride. J Wildl Dis. 1985;21:401.
28 John N, Leach JL, Rachana T, et al. Traumatic aneurysm of the occipital artery secondary to paintball injury. Clin Neurol Neurosurg. 2009;111:105.
29 Karlsoson T, Stahling S. Experimental blowgun injuries, ballistic aspects of modern blowguns. Forensic Sci Int. 2000;112:59.
30 Kay CN, Saunders TS, Pavan PR. Ocular injuries sustained in paintball trauma. Graefes Arch Clin Exp Ophth. 2010;248:331.
31 Kratz A, Levy J, Cheles D, et al. Airsoft gun related ocular injuries: Novel findings, ballistics investigation, and histopathologic study. Am J Ophthalmol. 2010;149:37.
32 Kuligod FS, Jirli PS, Kumar P. Air gun: a deadly toy? A case report. Med Sci Law. 2006;46:177.
33 Kulshrestha P, Munshi I, Wait R. Profile of chest trauma in a level I trauma center. J Trauma. 2004;57:576.
34 Lambrecht CB, Hargarten SW. Hunting-related injuries and deaths in Montana: The scope of the problem and a framework for prevention. J Wilderness Med. 1993;4:175.
35 Laraque D, Committee on Injury, Violence, and Poison Prevention. Technical report: Injury risk of nonpowder guns. Pediatrics. 2004;114:1357.
36 Lawrence HS. Fatal nonpowder firearm wounds: Case report and review of the literature. Pediatrics. 1990;85:177.
37 Lindsey D. The idolatry of velocity, or lies, damn lies and ballistics. J Trauma. 1980;20:1068.
38 Listman DA. Paintball injuries in children: More than meets the eye. Pediatrics. 2004;113:1518.
39 Lucas RM, Mitterer D. Pneumatic firearm injuries: Trivial trauma or perilous pitfalls? J Emerg Med. 1990;8:433.
40 Metz M, Kross M, Abt P, et al. Tree stand falls: A persistent cause of sports injury. South Med J. 2004;97:715.
41 Mouzopoulos G, Tzurbakis M. Unusual cervical spine injury by fishing harpoon. Eur J Emerg Med. 2009;16:209.
42 National Safety Council. Accident facts 1987. Washington, DC: The National Safety Council; 1987.
43 Nguyen MH, Annest JL, Mercy JA, et al. Trends in BB/pellet gun injuries in children and teenagers in the United States, 1985-99. Inj Prev. 2002;8:185.
44 North American Association of Hunter Safety Coordinators. Hunting accident report, with graphics of 1983-1987 data. Seattle: Outdoor Empire; 1987.
45 Ohio Division of Wildlife. Ohio hunter safety education student handbook. Seattle: Outdoor Empire; 1981.
46 Philippe G, Angenot L. Recent developments in the field of arrow and dart poisons. J Ethnopharmacol. 2005;100:85.
47 Pryce D. Safe hunting. New York: David McKay; 1974.
48 Reishus AD. Injuries and illness of big game hunters in western Colorado: A nine year analysis. Wilderness Environ Med. 2007;18:20.
49 Shrestha T, Kopp B, Bisset NG. The Moraceae-based dart poisons of South America. J Ethnopharmacol. 1992;37:129.
50 Smith JL, Lengerich EJ, Wood GC. Injuries due to falls from hunter’s tree stands in Pennsylvania. Am J Prev Med. 2009;37:433.
51 Smith JL, Wood GC, Lengerich EJ. Hunting related shooting incidents in Pennsylvania. J Trauma. 2005;58:1987-1999.
52 Stromberg BV. Symptomatic lead toxicity secondary to retained shotgun pellets. J Trauma. 1990;30:356.
53 Stubbs SN, Pasque CB, Brown S, et al. Spinal cord injuries from falls from hunting tree stands in Oklahoma, 1988-1999. J Okla State Med Assoc. 2004;97:156.
54 Sykes LN, Champion HR, Fouty WJ. Dum-dums, hollow-points, and devastators: Techniques designed to increase wounding potential of bullets. J Trauma. 1988;28:618.
55 Tokdemir M, Türkçüoğlu P, Kafadar H, et al. Sudden death following a pellet injury. Brain Inj. 2007;21:997.
56 Urquhart CK, Hawkins ML, Howdieshell TR, et al. Deer stands: A significant cause of injury and mortality. South Med J. 1991;84:686.
57 US Department of the Interior, Fish and Wildlife Service. 1985 National survey of fishing, hunting and wildlife associated recreation. Washington, DC: US Government Printing Office; 1988.
58 US Department of Interior, Fish and Wildlife Service. Hunting statistics and economics. Washington DC: Government Printing Office; 2008.
59 Vander Salm TJ, Ellis N. Blowgun dart aspiration. J Thorac Cardiovasc Surg. 1986;91:930.
60 Walker ML, Poindexter JM, Stovall I. Principles of management of shotgun wounds. Surg Gynecol Obstet. 1990;170:97.
61 Walsh IR, Eberhart A, Knapp JF, et al. Pediatric gunshot wounds: Powder and nonpowder weapons. Pediatr Emerg Care. 1988;4:279.
62 Wintemute GJ, Kraus JF, Teret SP, et al. Unintentional firearm deaths in California. J Trauma. 1989;29:457.
63 Zajtchuk R, editor. The textbook of military medicine, vol 5. Washington, DC: Office of the Surgeon General, 1989.