[level-membership-for-internal-medicine-category]
41 Homonymous hemianopia
Salient features
History
• Patient bumps into things on one side and may have a history of traffic accidents where one side of the car is damaged without the patient realizing.
• Patient may insist that they have one ‘bad’ eye (remember blindness in one eye causes impairment of perceiving distances but the normal eye will provide a full field of vision on both sides and hence patient will not bump into objects).
• Reading difficulty (suggests that the visual defect splits the midline: if the defect is on the right side, patient is unable to scan along the line to the next word and hence reading is almost impossible, whereas when the defect is on the left side the patient cannot find the beginning of the next line).
• Determine whether the patient is aware of his/her defect (if the patient is aware of the visual defect, it is likely the defect ‘splits’ the macula and bisects the central field; if the patient is unaware and bumps into things, then the defect is either macular sparing or an attention hemianopia).
Examination
Advanced-level questions
Where is the lesion?
The lesion is in the optic tract and beyond (visual acuity is intact when the macula is spared). Figure 41.1 shows the sites of the lesions and the visual field effects.
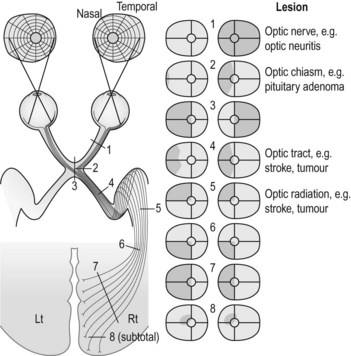
| Site | Type of homonymous hemianopia | |
|---|---|---|
| 1 | Optic nerve | Unilateral amaurosis |
| 2 | Lateral optic chiasm | Grossly incongruous, contralateral |
| 3 | Central optic chiasm | Bitemporal hemianopia |
| 4 | Optic tract | Incongruous, incomplete |
| 5 | Temporal lobe | Superior quadrantic defect, congruous partial or complete (contralateral) |
| 6 | Posterior parietal lobe | Inferior quadrantic defect, congruous partial or complete |
| 7 | Complete parieto-occipital interruption of the optic radiation | Complete congruous homonymous hemianopia with shift of foveal point, often sparing central vision |
| 8 | Incomplete damage to the visual cortex | Congruous homonymous scotomas, usually encroaching at least acutely on central vision |
[/level-membership-for-internal-medicine-category][not-level-membership-for-internal-medicine-category]
41 Homonymous hemianopia
Salient features
History
• Patient bumps into things on one side and may have a history of traffic accidents where one side of the car is damaged without the patient realizing.
• Patient may insist that they have one ‘bad’ eye (remember blindness in one eye causes impairment of perceiving distances but the normal eye will provide a full field of vision on both sides and hence patient will not bump into objects).
• Reading difficulty (suggests that the visual defect splits the midline: if the defect is on the right side, patient is unable to scan along the line to the next word and hence reading is almost impossible, whereas when the defect is on the left side the patient cannot find the beginning of the next line).
• Determine whether the patient is aware of his/her defect (if the patient is aware of the visual defect, it is likely the defect ‘splits’ the macula and bisects the central field; if the patient is unaware and bumps into things, then the defect is either macular sparing or an attention hemianopia).
