40 Holmes–Adie syndrome
Salient features
Examination
• The pupil is large, regular, irregular, oval, or circular
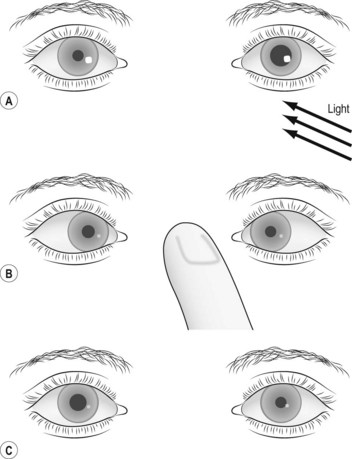
• The pupil will react sluggishly or fail to react to light (Fig. 40.1). However, if a strong and persistent stimulus is used it can be shown that the pupil contracts excessively to a very small size and when the stimulus is removed it returns to its former size gradually—this is known as the ‘myotonic’ pupil
• Delayed constriction in response to near vision
• Delayed re-dilatation after near vision
• Accomodation impaired (pupillary constriction secondary to accommodation is relatively less affected, because the ciliary muscle has innervation that is approximately 30 times as great as that of the iris sphincter)
• There is segmental palsy and segmental spontaneous movement of iris (Lancet 2000;356:1760–1)
• Proceed to check the ankle jerks and tell the examiner that you expect them to be absent. (The diminished reflexes result from dysfunction of the large sensory 1A afferent fibres involved in the spinal reflex arc, which is consistent with an underlying neuropathy.)
Questions
What is the significance of this condition?
It is benign and must not be mistaken for Argyll Robertson pupil.
Advanced-level questions
Where is the lesion in Adie’s tonic pupil?
It is caused by damage to the parasympathetic fibres from within the ciliary ganglion.
What is the difference between Adie’s tonic pupil and Holmes–Adie syndrome?
Adie’s tonic pupil with absent deep tendon jerks is called Holmes–Adie syndrome.
Which conditions may accompany this syndrome?
• Ross syndrome (segmental loss of sweating): the occurrence of Adie syndrome and segmental anhidrosis or hypohydrosis. It consists of cranial postganglionic parasympathetic and sympathetic dysfunction in association with more widespread autonomic failure that is rarely clinically relevant. The course is usually benign with a possible expansion of the dyshidrotic area.






