[level-membership-for-radiology-category] Small hypodense nodules may be microabscesses



• Stomach, small bowel, and large bowel
 Wall thickening raises concern for opportunistic infection, which can involve any segment of GI tract
Wall thickening raises concern for opportunistic infection, which can involve any segment of GI tract
Wall thickening raises concern for opportunistic infection, which can involve any segment of GI tract


• Lymph nodes






 involving retroperitoneal and mesenteric nodes. Biopsy confirmed MAI.
involving retroperitoneal and mesenteric nodes. Biopsy confirmed MAI.
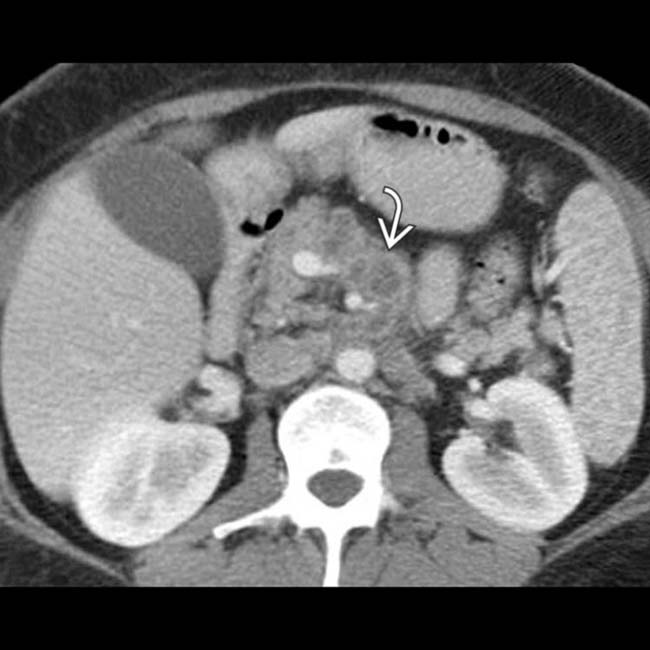
 . This constellation of findings was found to represent disseminated mycobacterial infection.
. This constellation of findings was found to represent disseminated mycobacterial infection.IMAGING
General Features








CT Findings
• Liver
 Liver may appear nodular and cirrhotic due to strong demographic overlap of HIV and chronic viral hepatitis
Liver may appear nodular and cirrhotic due to strong demographic overlap of HIV and chronic viral hepatitis
 Small hypodense nodules scattered throughout liver suggests microabscesses (often due to Mycobacterium avium-intracellulare [MAI], tuberculosis, histoplasmosis, Candida, Pneumocystis, etc.)
Small hypodense nodules scattered throughout liver suggests microabscesses (often due to Mycobacterium avium-intracellulare [MAI], tuberculosis, histoplasmosis, Candida, Pneumocystis, etc.)
Liver may appear nodular and cirrhotic due to strong demographic overlap of HIV and chronic viral hepatitis Small hypodense nodules scattered throughout liver suggests microabscesses (often due to Mycobacterium avium-intracellulare [MAI], tuberculosis, histoplasmosis, Candida, Pneumocystis, etc.)


• Biliary tree


• Spleen
 Small tiny hypodense foci (microabscesses) usually due to disseminated infection (e.g., Candida, MAI, tuberculosis, coccidioidomycosis, Pneumocystis, etc.)
Small tiny hypodense foci (microabscesses) usually due to disseminated infection (e.g., Candida, MAI, tuberculosis, coccidioidomycosis, Pneumocystis, etc.)
 Small tiny hypodense foci (microabscesses) usually due to disseminated infection (e.g., Candida, MAI, tuberculosis, coccidioidomycosis, Pneumocystis, etc.)
Small tiny hypodense foci (microabscesses) usually due to disseminated infection (e.g., Candida, MAI, tuberculosis, coccidioidomycosis, Pneumocystis, etc.)

• Stomach, small bowel, and large bowel
 Bowel wall thickening, mucosal hyperemia, and fat stranding surrounding bowel should always raise concern for infection (including opportunistic infections)
Bowel wall thickening, mucosal hyperemia, and fat stranding surrounding bowel should always raise concern for infection (including opportunistic infections)
 Most opportunistic infections can involve any segment of GI tract (Cryptosporidium, CMV, MAI, tuberculosis, microsporidium, Clostridium difficile, amebiasis, etc.)
Most opportunistic infections can involve any segment of GI tract (Cryptosporidium, CMV, MAI, tuberculosis, microsporidium, Clostridium difficile, amebiasis, etc.)
 Mural thickening of esophagus suggests esophagitis, often due to candidiasis, CMV, or herpes simplex
Mural thickening of esophagus suggests esophagitis, often due to candidiasis, CMV, or herpes simplex
Bowel wall thickening, mucosal hyperemia, and fat stranding surrounding bowel should always raise concern for infection (including opportunistic infections)
Most opportunistic infections can involve any segment of GI tract (Cryptosporidium, CMV, MAI, tuberculosis, microsporidium, Clostridium difficile, amebiasis, etc.)


 Mural thickening of esophagus suggests esophagitis, often due to candidiasis, CMV, or herpes simplex
Mural thickening of esophagus suggests esophagitis, often due to candidiasis, CMV, or herpes simplex

• Lymph nodes
 Mild generalized lymphadenopathy (< 1.5 cm) is usually reactive and may be 1st clue to HIV infection
Mild generalized lymphadenopathy (< 1.5 cm) is usually reactive and may be 1st clue to HIV infection
Mild generalized lymphadenopathy (< 1.5 cm) is usually reactive and may be 1st clue to HIV infection


• Kidney




Ultrasonographic Findings
• Kidney



• Gallbladder











PATHOLOGY
General Features
• Etiology
 HIV-infected patients have an increased risk of developing malignancies, particularly when coinfected by Epstein-Barr virus, herpesvirus, or papillomavirus
HIV-infected patients have an increased risk of developing malignancies, particularly when coinfected by Epstein-Barr virus, herpesvirus, or papillomavirus
 Infections more common in HIV patients even with CD4 counts > 200, although risk increases substantially with lower CD4 counts
Infections more common in HIV patients even with CD4 counts > 200, although risk increases substantially with lower CD4 counts
 HIV-infected patients have an increased risk of developing malignancies, particularly when coinfected by Epstein-Barr virus, herpesvirus, or papillomavirus
HIV-infected patients have an increased risk of developing malignancies, particularly when coinfected by Epstein-Barr virus, herpesvirus, or papillomavirus
– Incidence of AIDS-defining malignancies (AIDS-related non-Hodgkin lymphoma, Kaposi sarcoma) has dramatically ↓ with antiretroviral therapy
– Risk of other malignancies, which are often atypically aggressive and occur at younger ages than normal, still higher in HIV patients



 Infections more common in HIV patients even with CD4 counts > 200, although risk increases substantially with lower CD4 counts
Infections more common in HIV patients even with CD4 counts > 200, although risk increases substantially with lower CD4 counts











CLINICAL ISSUES
Presentation
• Most common signs/symptoms












 , which is markedly echogenic, compatible with the patient’s known HIV nephropathy. Unlike other forms of chronic renal failure, the kidneys in HIV nephropathy are often normal in size or enlarged.
, which is markedly echogenic, compatible with the patient’s known HIV nephropathy. Unlike other forms of chronic renal failure, the kidneys in HIV nephropathy are often normal in size or enlarged.
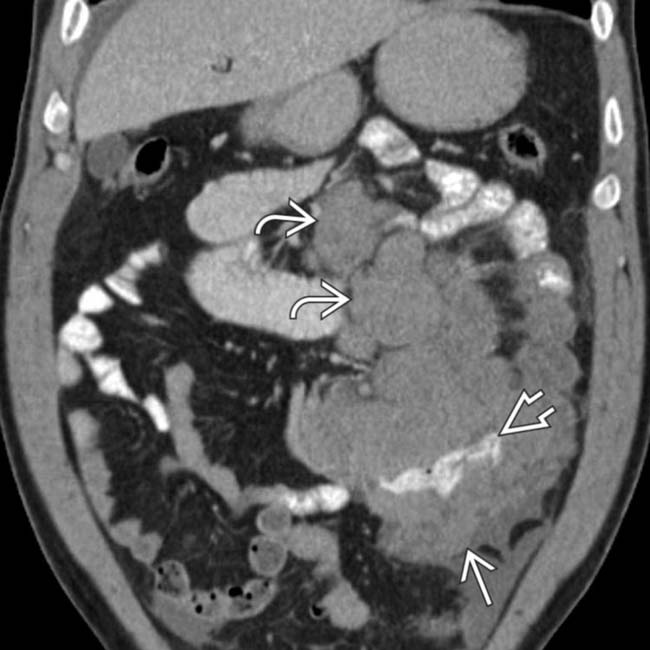
 in the left lower quadrant with internal enteric contrast
in the left lower quadrant with internal enteric contrast  . Note the extensive lymphadenopathy
. Note the extensive lymphadenopathy  more superiorly. These findings are compatible with the patient’s biopsy-proven AIDS-related non-Hodgkin lymphoma.
more superiorly. These findings are compatible with the patient’s biopsy-proven AIDS-related non-Hodgkin lymphoma.
 found to represent AIDS-related non-Hodgkin lymphoma.
found to represent AIDS-related non-Hodgkin lymphoma.
 , including a mass with internal hemorrhage
, including a mass with internal hemorrhage  , which were proven to be non-Hodgkin lymphoma. An unusual feature in this case is the mild obstruction of the intrahepatic bile ducts
, which were proven to be non-Hodgkin lymphoma. An unusual feature in this case is the mild obstruction of the intrahepatic bile ducts  .
.
 . Biopsy revealed this to represent AIDS-related B-cell non-Hodgkin lymphoma.
. Biopsy revealed this to represent AIDS-related B-cell non-Hodgkin lymphoma.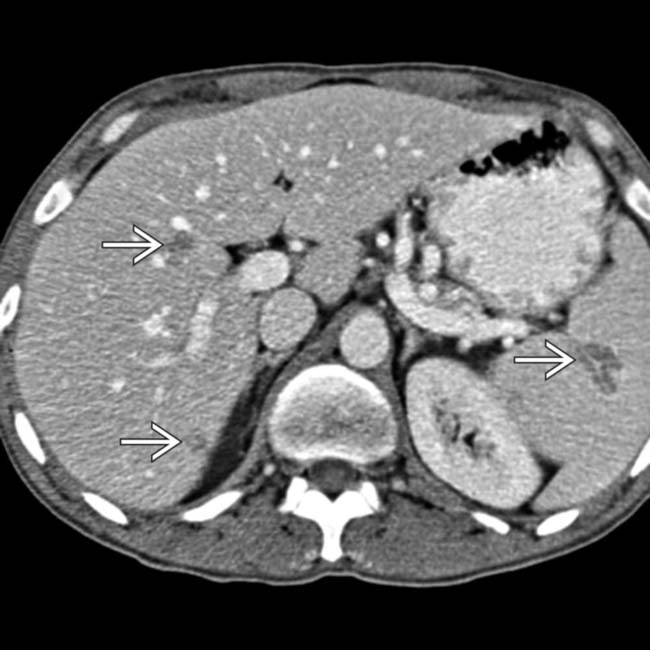
 in the liver and spleen.
in the liver and spleen.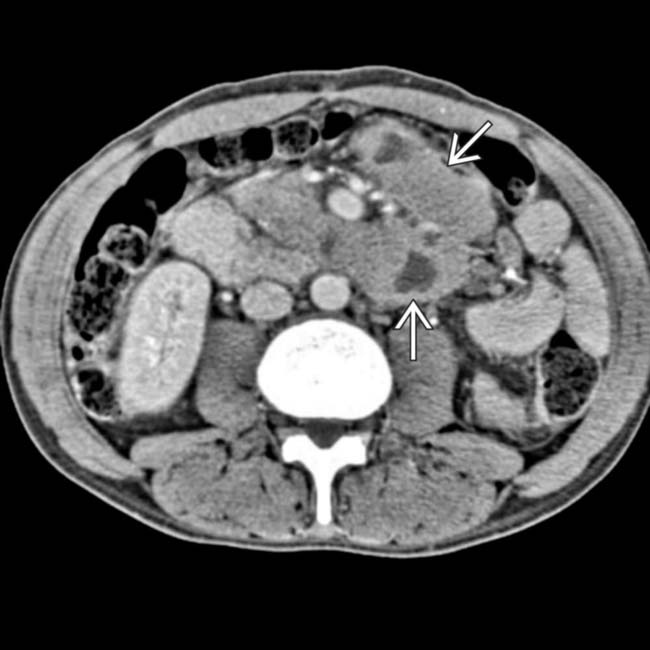
 , these seen in the abdominal nodes. These findings were found to reflect non-Hodgkin lymphoma.
, these seen in the abdominal nodes. These findings were found to reflect non-Hodgkin lymphoma.
 , with many of the nodes having a hyperdense (hypervascular) appearance characteristic of involvement by Kaposi sarcoma.
, with many of the nodes having a hyperdense (hypervascular) appearance characteristic of involvement by Kaposi sarcoma.
 of this patient.
of this patient.
 within the left kidney, due to healed infection with Pneumocystis carinii.
within the left kidney, due to healed infection with Pneumocystis carinii.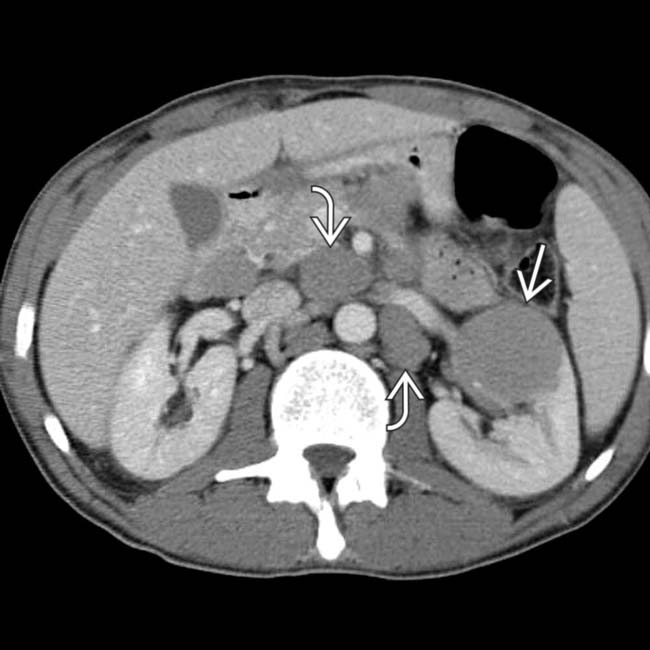
 in the kidney with multiple enlarged abdominal nodes
in the kidney with multiple enlarged abdominal nodes  in a patient with AIDS-related lymphoma.
in a patient with AIDS-related lymphoma.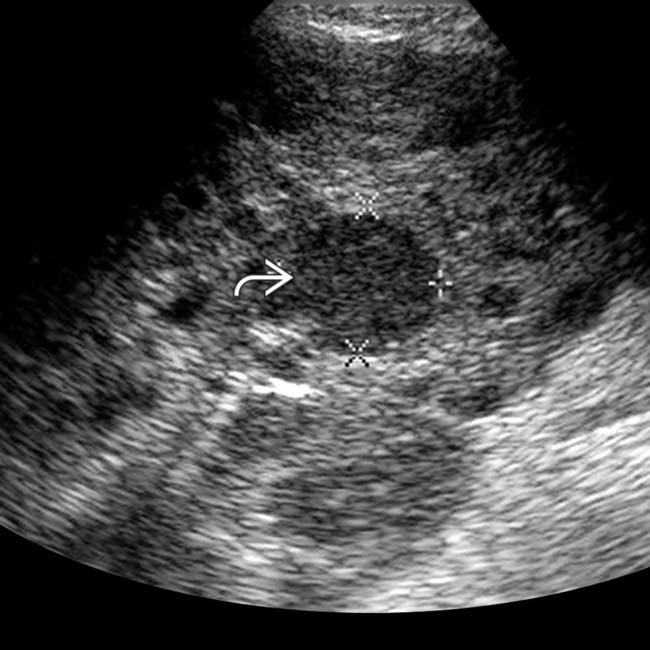
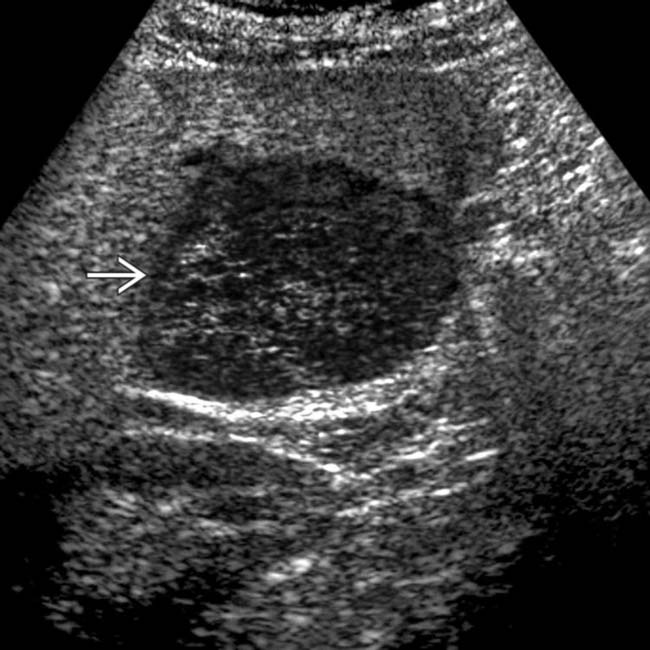
 in the spleen. The imaging findings on ultrasound are nonspecific, but this was biopsied and shown to represent non-Hodgkin lymphoma.
in the spleen. The imaging findings on ultrasound are nonspecific, but this was biopsied and shown to represent non-Hodgkin lymphoma.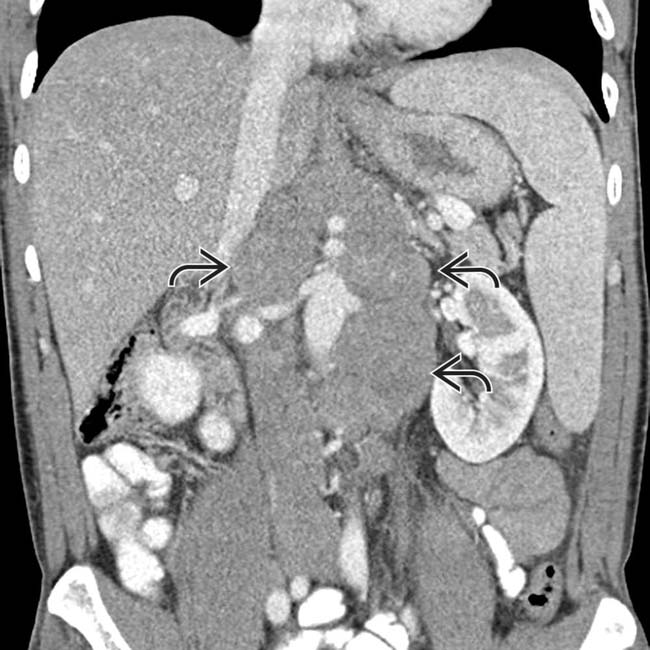
 , found to represent AIDS-related non-Hodgkin lymphoma.
, found to represent AIDS-related non-Hodgkin lymphoma.

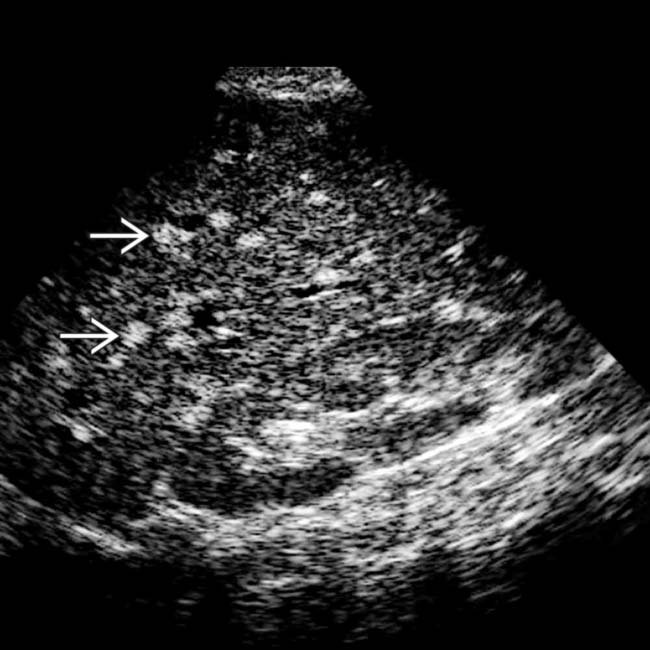
 in the right upper quadrant. This was found to be chronic MAI infection.
in the right upper quadrant. This was found to be chronic MAI infection.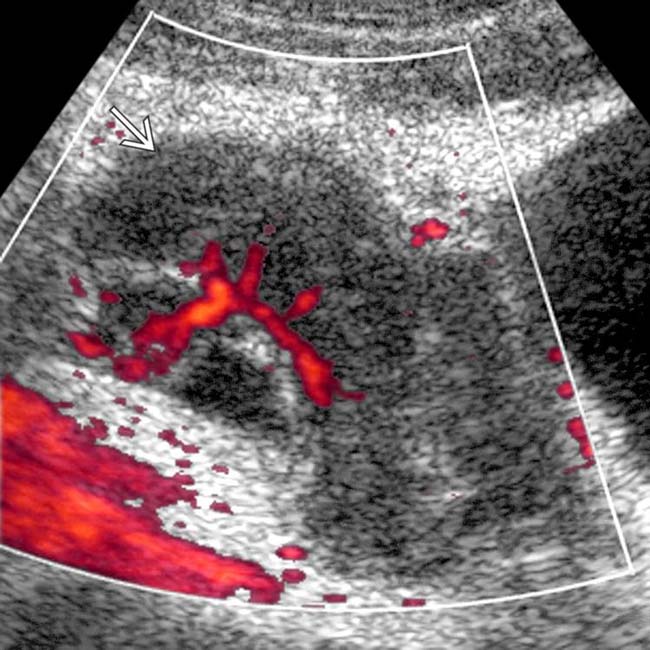
 just anterior to the bladder, with prominent internal flow.
just anterior to the bladder, with prominent internal flow.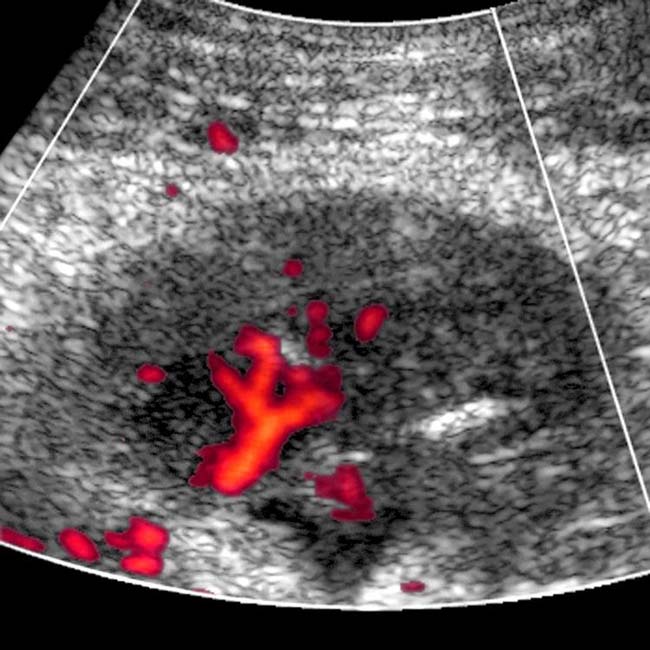
 within the liver. These are healed, calcified granulomas that have resulted from hepatic infection with Mycobacterium avium complex.
within the liver. These are healed, calcified granulomas that have resulted from hepatic infection with Mycobacterium avium complex.
 , with many of the nodes having a hyperdense (hypervascular) appearance that is characteristic of involvement by Kaposi sarcoma.
, with many of the nodes having a hyperdense (hypervascular) appearance that is characteristic of involvement by Kaposi sarcoma.[/level-membership-for-radiology-category][not-level-membership-for-radiology-category]&
Buy Membership for Radiology Category to continue reading. Learn more here
[/not-level-membership-for-radiology-category]
