[level-membership-for-pediatrics-category]
CHAPTER 20 Hirschsprung Disease
Swenson Pull-Through Procedure
Step 1: Surgical Anatomy
Step 2: Preoperative Considerations
Neonates



Infants and Children
Management
Step 3: Operative Steps
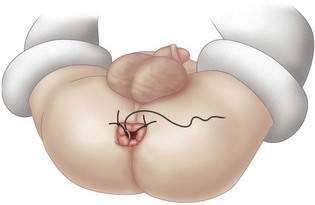
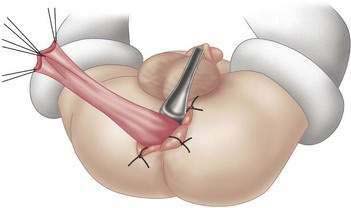
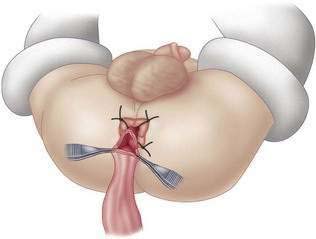
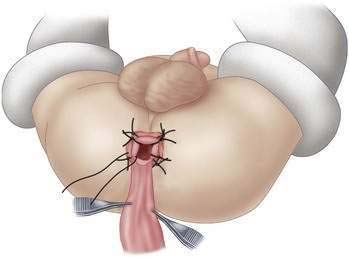
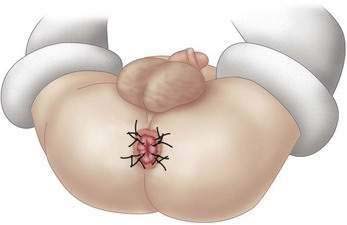
Transanal Operative Technique
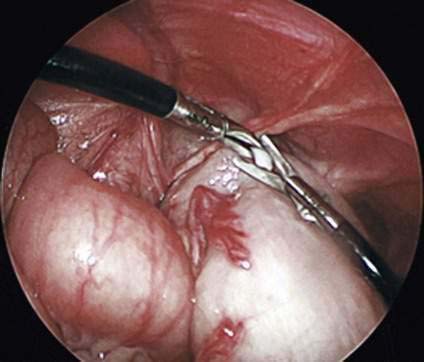
Operative Technique: Minimally Invasive Assisted
Step 4: Postoperative Care
Follow-up Care
Step 5: Pearls and Pitfalls
Curran TJ, Raffensperger JG. The feasibility of laparoscopic Swenson pull-through. J Pediatr Surg. 1994;29(9):1273-1275.
Curran TJ, Raffensperger JG. Laparoscopic Swenson pull-through: a comparison with the open procedure. J Pediatric Surg. 1996;31(8):1155-1157.
Dasgupta R, Langer JC. Transanal pull-through for Hirschsprung’s disease. Semin Pediatr Surg. 2005;14(1):64-71.
Nishijima E, Kimura K, Tsugawa C, Muraji T. The colon patch graft procedure for extensive aganglionosis: long-term follow-up. J Pediatr Surg. 1998;33(2):215-219.
Swenson O. Hirschsprung’s disease. In: Raffensperger JG, editor. Swenson’s pediatric surgery. 4th ed. New York: Appleton-Century-Crofts; 1980:507-531.
Teitelbaum DH, Coran AG. Hirschsprung’s disease and related neuromuscular disorders of the intestine, 6th ed. Grosfeld JL, O’Neill JA, Fonkalsrud EW, Coran AG, editors. Pediatric surgery, vol. 2, 2006. Elsevier, Philadelphia:1514-1559
Weidner BC, Waldhausen JH. Swenson revisited: a one-stage, transanal pull-through procedure for Hirschsprung’s disease. J Pediatr Surg. 2003;38(8):1208-1211.
[/level-membership-for-pediatrics-category][not-level-membership-for-pediatrics-category]
CHAPTER 20 Hirschsprung Disease
Swenson Pull-Through Procedure
Step 1: Surgical Anatomy
Step 2: Preoperative Considerations
Neonates
Infants and Children
Management
[/not-level-membership-for-pediatrics-category]
