CHAPTER 19 Hirschsprung Disease
Soave (Open and Laparoscopic-Assisted) and Duhamel Techniques
Open Endorectal (Soave) Pull-Through
Step 1: Surgical Anatomy
♦ The endorectal pull-through procedure essentially requires the removal of the rectal mucosa and submucosa to create an aganglionic cuff through which normal ganglionic intestine is brought through. In most cases, this can be performed as a primary or one-stage procedure, avoiding the need for a leveling colostomy. Advantages of an endorectal dissection include the avoidance of trauma to sensory nerves in the rectum and preservation of the internal sphincter.
♦ To have a complete understanding of the surgical anatomy, some consideration should be given to the histology of the colon.




♦ The muscular complex surrounding the anal canal includes the internal sphincter arising as the continuation of the circular smooth muscle of the rectum; this ends 2.6 to 6.6 mm caudal to the dentate line. Surrounding this layer is a striated muscular complex called the levator ani, contiguous with the external sphincter that begins just caudal to the internal sphincter. Therefore, the endorectal mucosal dissection should continue to 5 mm cranial to the dentate line in a neonate and 1 cm above this line in older children. By maintaining this distance, the entire sphincteric complex is easily spared from inadvertent damage, decreasing the risk of incontinence.
Step 2: Preoperative Considerations
♦ Even in neonates, serial rectal washouts should be performed with 10 mL/kg of normal saline accompanied by digital dilation. It should be emphasized that these are washouts, not enemas. This requires that a large-bore catheter be placed above the aganglionic region and left in place to allow the evacuation of stool. The fluid for or the irrigation performed most immediately before the operation should also include 1% neomycin. In addition, parenteral antibiotics covering both skin flora and enteric organisms should be administered within a half hour of initial incision as well as two doses postoperatively.
♦ Older infants and children should also undergo a formal bowel preparation. Two days before surgery, a clear liquid diet should be initiated. On the day before surgery, a polyethylene glycol (PEG ~3500 molecular weight) oral solution should be given. Because children with Hirschsprung disease cannot spontaneously evacuate stool, serial rectal washouts must be performed every 4 to 6 hours on the day the PEG solution is administered.
Step 3: Operative Steps
Positioning and Preparation
♦ A nasogastric tube is placed after induction of anesthesia. The patient should be placed in lithotomy position, with the buttocks brought to the edge of the table and propped on a folded towel. The legs should be carefully positioned on wooden skis or leg supports with proper padding and care paid to pressure points. Both the abdomen and perineum should be prepared with antiseptic solution in standard fashion before draping both areas to allow for access to the anus and entire abdomen. Alternatively, in infants, the entire body from the upper abdomen to the feet may be prepped in total, and feet and legs placed in stockinettes (Fig. 19-1). One may then have an assistant elevate both legs during the transanal anastomosis portion of the procedure. Once the patient is prepped, a Foley catheter should be inserted into the urinary bladder. Before the incision is made, the entire table should be placed in a slight Trendelenburg position.

Leveling
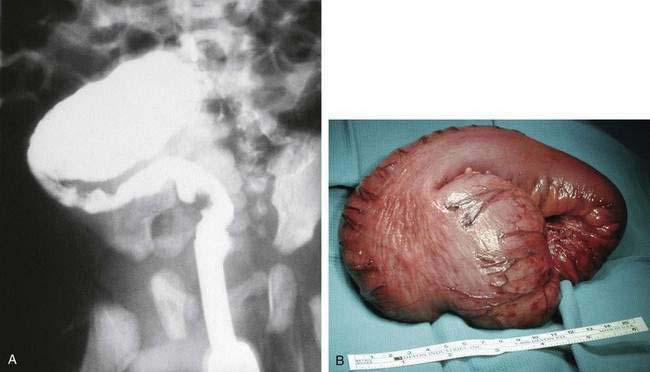
♦ The classic appearance of the proximal (ganglionic) bowel shows an extremely hypertrophied muscular wall, with a loss of the taenia coli (Fig. 19-2). The transition zone between aganglionic and ganglionic bowel can be made by a combination of visual inspection and a series of frozen sections. Once the presence of normal ganglion cells is identified, the bowel should be transected with a stapling device above the transition zone (ideally about 5 cm proximal or cranial to this point). This step is recommended because the level of aganglionosis can vary around the circumference of the colon, and proceeding more proximally will help to ensure that the selected bowel will have essentially normal pathology throughout. Both the proximal bowel and distal bowel are then mobilized, with the latter dissected to around 2 to 4 cm above the peritoneal reflection. Traction sutures are then placed at the end of the proximal colonic segment to facilitate the pull-through.
Endorectal Dissection
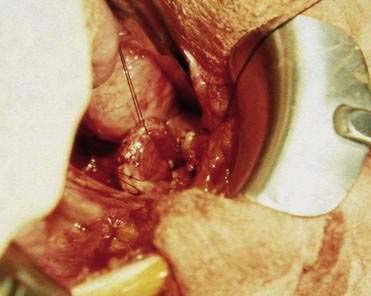
♦ Beginning on the distal bowel, a 2-cm segment just below the level of the peritoneal reflection should be cleared of serosa, mesentery, and pericolonic fat. The seromuscular layer is then incised by electrocautery down to the level of the submucosa. This incision is extended circumferentially using a hemostat. Dissection is carried further using a Kitner to perform blunt dissection, or in infants or neonatal patients a cotton-tipped applicator can be used effectively for this purpose (Fig. 19-3).
♦ Once established, this plane of dissection is continued distally. Upward pulling on the traction sutures of the distal rectum is necessary to provide helpful countertraction. A helpful addition is the placement of other traction sutures into each quadrant of the muscle cuff as the dissection progressively develops (Fig. 19-4). Without the application of this countertraction, the dissection becomes ineffective, and one cannot proceed distally to an adequate level. Electrocautery should be used to coagulate larger communicating vessels between the submucosa and muscular cuff. The dissection should be carried out to within 0.5 cm of the dentate line in neonates and approximately 1 cm in older children.
♦ Of note, this dissection can be carried out via a transanal approach, but if the dissection is begun transabdominally, it is most easily continued in this manner to maintain the proper plane. In addition, employment of the transabdominal approach minimizes the stretch placed on the anal sphincters by the retractors required to provide exposure. Once the dissection is complete, the posterior portion of the muscular cuff is split posteriorly and carried down as distally as possible, almost to the same level as the endorectal dissection.

Pull-Through
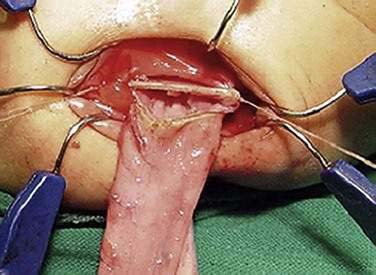
♦ At this point, one surgeon moves to the perineal field and places retractors (phrenic or army-navy) at the anal verge. A ring forceps or Kelly clamp is then inserted into the rectum, and the assistant in the abdominal field will place the end of the mucosal or submucosal tube into the clamp. Eversion of the dissected segment is then performed, and the end of the tube is regrasped with a clamp and held in traction (Fig. 19-5).

Anastomosis
♦ An incision should then be made on the anterior half of the mucosal or submucosal tube, 0.5 cm proximal to the dentate line. A Kelly clamp should be placed through this opening and used to grasp the traction sutures on the proximal bowel (Fig. 19-6). Particular attention should be paid to avoid twisting the bowel as it is pulled through the muscular cuff. The placement of two differently colored sutures on the mesenteric and anti-mesenteric sides of the ganglionic bowel will help the surgeon identify and correct any twisting that may occur during the pull-through process.
♦ The anastomosis is begun by incising the anterior half of the ganglionic colon and suturing it to the anterior cuff of the anal mucosa using 4-0 polyglactin suture. Sutures placed at each corner and in midline are then used as traction sutures by the assistant as the surgeon places interrupted sutures to complete the anastomosis quadrant by quadrant.
♦ The posterior portion of the anastomosis should be completed by incising one quarter of the remaining ganglionic colon and everted mucosal or submucosal segment.
♦ Exposure by the assistant is facilitated by outward traction placed on the sutures that have been placed into each quadrant.
♦ The final quadrant of the anastomosis should be completed and inspected. The neo-rectum can be inverted by applying gentle upward traction on the colon. Rectal examination can then be performed to palpate the anastomosis 1.5 to 2 cm proximal to the anal verge. After a change of gloves, attention should be redirected to the abdominal field.
Step 4: Postoperative Care
♦ The nasogastric tube can typically be removed at the end of the operation. Care following the endorectal pull-through is that practiced for any patient who has undergone colon resection with a low anastomosis. It is advisable to allow no rectal examinations or medications per rectum for at least 2 to 3 weeks. All attempts should be made to provide postoperative pain relief, as well as to normalize diet and provide stool softeners as soon as possible. As mentioned previously, two doses of antibiotics with skin and enteric flora coverage should be administered postoperatively. Follow-up and careful calibration of the anastomosis with Hegar dilators should be performed at frequent clinic visits beginning at 3 weeks postoperatively.
Step 5: Pearls and Pitfalls
♦ A general way to determine adequate mobilization of the proximal colonic segment is to stretch it over the pubis to the anal verge. If more length is needed, it may be helpful to divide the inferior mesenteric artery near its origin, preserving the marginal arterial arcade.
♦ Concern over the subsequent problems with stool evacuation caused by the presence of an abnormally functioning internal anal sphincter has led some surgeons to divide not only the posterior wall of the muscular cuff but also the cranial portion of the internal sphincter. This appears to cause few, if any, problems with continence.
♦ As mentioned, it is helpful to use different colored sutures on the end of the proximal, ganglionic bowel to maintain its orientation.
♦ Although complete strictures of the anastomosis are uncommon, the anastomosis should be gently sized with a Hegar dilator at each clinic visit. In general, at the initial visit (about 3 weeks postoperatively), a neonatal pull-through should accept a size 7 to 9 Hegar. Subsequent visits should gradually increase this size to between 10 and 12.
Laparoscopic-Assisted Endorectal (Soave) Pull-Through
Step 2: Preoperative Considerations
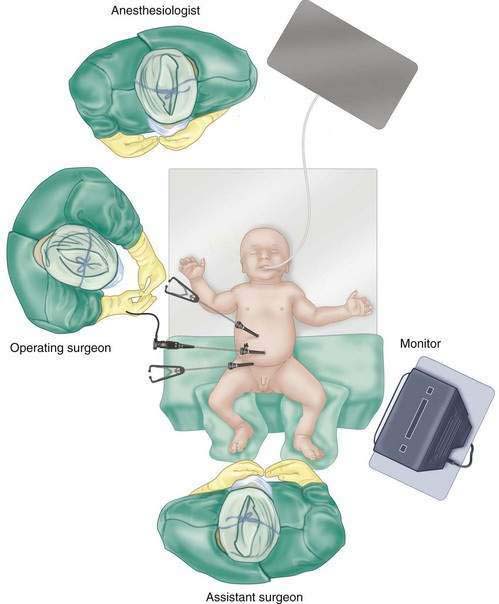
♦ Preoperative washouts and, depending on the patient’s age, bowel preparation are identical to that for the endorectal pull-through, as detailed above. Use of preoperative antibiotics is the same as that with the open endorectal pull-through. Careful consideration should be given to positioning, for if the lower extremities are too high, they will interfere with the surgeon’s ability to manipulate the laparoscopic instruments. It is often easier to prep the entire lower half of the infant into the operative field, and keep the legs in a supine position, or hanging just off the bed, during the laparoscopic portion of the procedure. One could then have an assistant elevate the lower extremities once the surgeons are ready to perform the perineal portion of the procedure.
Step 3: Operative Steps
Leveling
♦ Before mobilization of the colon, it is necessary to determine the level of aganglionosis, which begins by visually inspecting for a transition zone and taking a seromuscular biopsy just above this level. This is most easily accomplished by grasping the serosa with the nondominant hand and sharply cutting into the intestinal wall until the level of the submucosa is reached. One then proceeds to dissect the bowel bluntly in this plane until a 0.5-cm piece of muscularis is obtained. If a perforation occurs, one can simply close this hole with an intracorporeally placed suture.
♦ If one cannot identify a transition zone, one should take the first biopsy just above the peritoneal reflection and proceed proximally at about 10-cm intervals as needed. One should also consider performing an appendectomy early in such a case, particularly if specimens continue to show absence of ganglia, as the child may have total colonic aganglionosis.
Dissection
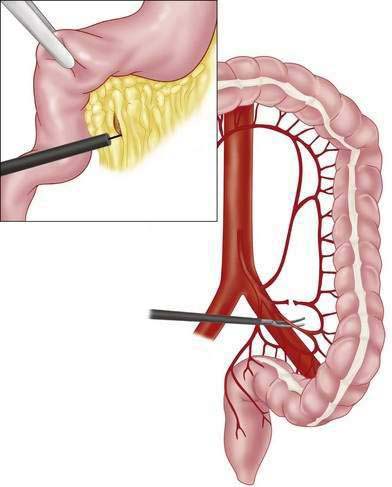
♦ Dissection and leveling of the aganglionic segment proceed as in the open technique, with the assistant holding the camera and the upper trocar grasping the rectum for exposure and retraction. Surgical clip appliers may be used to ligate blood vessels, with small vessels controlled by cautery (Fig. 19-8). Following mobilization, the surgeon and assistant should switch places. The transanal dissection, pull-through, and anastomosis then proceed, the details of which are given in the chapter on the transanal approach (see Chapter 18).
Step 5: Pearls and Pitfalls
♦ Ideally the two working ports should each be a hand’s width away from the umbilical port; however, if the inferior port is placed too low, the mobility of the trocar will be limited by the lower extremities and iliac crest. An ideal way to assess whether one has achieved adequate mobilization of the ganglionic bowel is to confirm that it can be easily be pulled down to the lowest portion of the pelvis before beginning the transanal dissection.
Duhamel Pull-Through
Step 1: Surgical Anatomy
♦ The Duhamel technique was advanced in 1956 to avoid the tedious pelvic dissection of the Swenson procedure and to protect the nervi erigentes, which may be found lateral and anterior to the rectum. The procedure has undergone several modifications, the most important of which was by Martin, and included the use of an automatic stapling device. It is fairly straightforward and continues to be popular today. Despite its relative simplicity, several key technical points must be followed.
♦ As with other pull-through procedures, ganglionic bowel is brought down to less than 1 cm proximal to the dentate line. To preserve the autonomic nerve plexus to the genitourinary system, very little manipulation of the rectum is performed anteriorly.
♦ In the past, the child often had a leveling colostomy, which was placed several months previously. This served to decompress the bowel and return it to normal caliber. The operation was generally performed when the child was 6 to 12 months of age with a weight of 10 kg. With the use of smaller endo-stapling devices, the procedure can also be performed primarily in the newborn period.
Step 2: Preoperative Considerations
♦ The child is admitted the day before the surgery for a mechanical bowel preparation as well as oral antibiotics. Care must be taken to give adequate rectal and colonic washouts because stool is often inspissated in the distal rectum. It is necessary to do a rectal examination on the child before the pull-through to ensure that no residual stool is present. Preoperative antibiotics should be given.
♦ A nasogastric tube is placed after induction of anesthesia. The child is placed in a supine position, and the patient is prepared circumferentially from the abdomen to the feet. Stockinettes are placed around each foot, and a Foley catheter is inserted into the bladder after the patient has been prepared and draped. Excellent exposure is obtained by assistants supporting and flexing the lower extremities at the hips during the anal anastomosis. Alternatively, the child can be placed in stirrups or on skis.
Step 3: Operative Steps
Leveling
♦ The transition zone between aganglionic and ganglionic bowel can be made by a combination of visual inspection and a series of frozen sections. Once the presence of normal ganglion cells is identified, the bowel should be transected with a stapling device above the transition zone (ideally approximately 5 cm proximal or cranial to this point) to ensure that the remaining bowel will have essentially normal innervation. Both the proximal bowel and distal bowel are then mobilized, with the latter mobilized to approximately 2 to 4 cm above the peritoneal reflection. Traction sutures are then placed at the end of the proximal colonic segment to facilitate the pull-through.
Retrorectal Dissection
♦ Blunt dissection in the posterior midline is used to create a retrorectal space down to the level of the pelvic floor. Dissection is considered complete once an assistant’s finger, inserted only 1 to 1.5 cm into the anus, can be palpated from the abdominal field. While a blunt clamp may help the dissection, an index finger can easily be used to develop this plane.
Pull-Through
♦ If the legs are not already in skis, they should be drawn upward by an assistant to allow a clear view of the anus. The surgeon should move to the perineal portion of the surgical field and place narrow anal retractors to be held by assistants in the abdominal field. Although the instruments used in the perineal portion of the procedure should be treated as contaminated, there is no need to maintain a separate sterile field with separate setups. However, gloves should be changed once the anastomosis is created.
♦ Cautery is used to create a full-thickness incision on the posterior wall of the rectum, 0.5 cm (1 cm in older infants) proximal to the dentate line. This distance should be carefully maintained by curving the incision appropriately when extended in each direction. To maintain proper orientation of the bowel, the inferior and superior edges of the incision are respectively marked with undyed and dyed polyglactin sutures. These sutures are placed in the midline, and with one on each edge; hemostats are used to hold each suture in position.
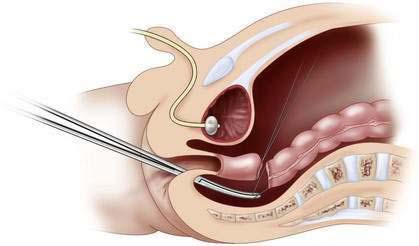
♦ From the perineal field, a long clamp is inserted into the retrorectal space and toward the abdominal field. The clamp is used to grasp the tacking sutures on the distal ganglionic bowel, and the surgeon in the abdominal field guides the bowel to help prevent rotation of the bowel as it is pulled through (Fig. 19-9).
♦ The staple line is then excised on the anterior half of the ganglionic colon, and a single-layered anastomosis is begun using the three previously placed polyglactin sutures. Each stitch should be carefully placed to ensure that the anterior wall of the anus is not incorporated into any of the sutures.
Anastomosis
♦ After completing the anterior half of the anastomosis, the remainder of the staple line is excised, and the anastomosis is completed.
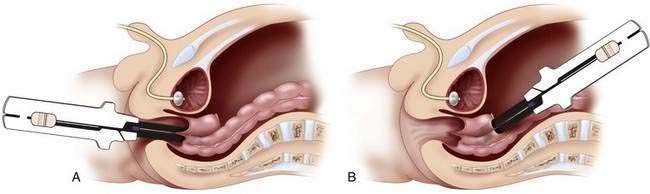
♦ One arm of an automatic stapling device is placed into the native anal canal while the other is placed into the neorectum (Fig. 19-10). The stapler is fired directly in the midline, and the suture line is checked for hemostasis. A long (80 mm) stapling device is generally preferred; a smaller endo-stapler is used in newborns.
♦ It is common for a single staple application to be insufficient to complete the full length of the anastomosis of ganglionic and aganglionic bowel (Fig. 19-10, B). This can be remedied by firing the stapler from the abdominal field. The staple line of the aganglionic rectum is opened, and a small enterotomy is made in the ganglionic colon at a similar level to allow placement of a reloaded stapler. The anastomosis must be digitally examined to ensure that it is complete. Huge fecalomas can form if a bridge or spur remains between bowel segments.
♦ The opened staple line is then sutured to the enterotomy in the ganglionic colon in two layers. Care is taken not to leave a blind-ending stump of aganglionic bowel because this could lead to the development of a large fecaloma. The neorectum may or may not be reperitonealized, and the abdomen is closed. The nasogastric tube typically can be removed at the end of the procedure.
Aldridge RT, Campbell PE. Ganglion cell distribution in the normal rectum and anal canal: a basis for the diagnosis of Hirschsprung’s disease by anorectal biopsy. J Pediatr Surg. 1968;3:475-490.
Teitelbaum DH, Coran AG. Hirschsprung disease, operations. In: Spitz L, Coran AG, editors. Operative pediatric surgery. 6th ed. London: Hodder Headline Group; 2006:553-563.
Teitelbaum DH, Coran AG. Hirschsprung’s disease and related neuromuscular disorders of the intestine. In: Grosfeld JL, O’Neil JA, Fonkalsrud EW, Coran AG, editors. Pediatric surgery. 6th ed. Philadelphia: Mosby Elsevier; 2006:1514-1547.





