[level-membership-for-radiology-category]
Hip & proximal femur
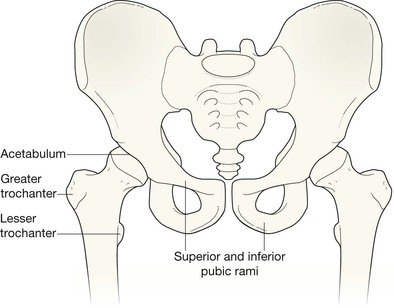
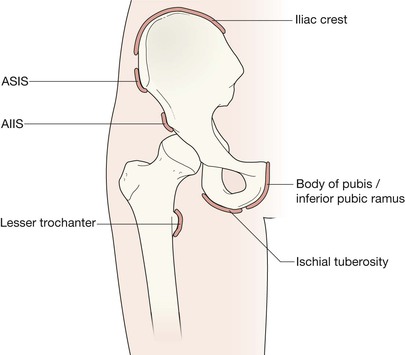
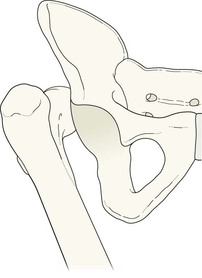
Normal anatomy
AP view
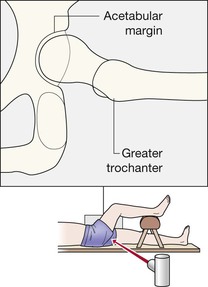
AP and lateral views
The femoral neck should:
The intertrochanteric region should:
Secondary centres (apophyses)
The femur and pelvis of an adolescent will show several small secondary centres (the apophyses).
Analysis: the checklists
Detailed inspection should focus on the specific clinical history. Thus…
An elderly patient has suffered a simple fall
Check for:
▪ A black line—a displaced fracture—across the femoral neck.
A few fractures are very difficult to detect. If the radiographs appear superficially normal it is important to check again and answer the following questions:
An adolescent patient has acute/chronic pain following athletic activity
Check that:
Patient of any age who has sustained high velocity trauma
Check all of the features described above and also check:
Hip pain in a young patient with no history of recent trauma
▪ Age 4–10 years: consider Perthe’s disease of the femoral head.
▪ Around the age of puberty: consider slipped capital femoral epiphysis.


Normal lateral view. The same patient as above. The two sites that must be checked are the neck of the femur and the trochanteric region. This peculiar projection might seem anatomically counterintuitive—see explanation on p. 228.
The common injuries
Elderly patient after a simple fall
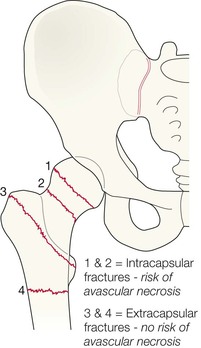
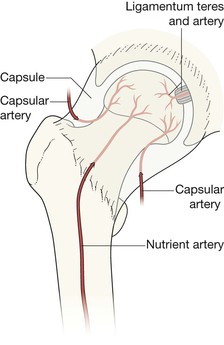
Femoral neck fracture
The most common cause of an acute orthopaedic admission in the elderly. A fall is not always a prerequisite. As the hip twists (eg during a stumble) a rotational force can occur, causing a fracture through osteoporotic bone.
Fractures of the femoral neck and proximal femur1,2 occur at characteristic sites. Approximately 50% of all hip fractures are trochanteric3.
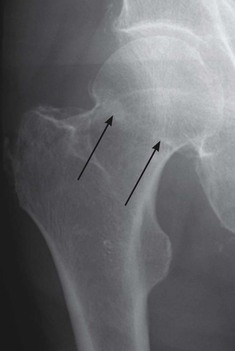
Approximately 95% of hip fractures are widely displaced and easy to detect. A few are very difficult to detect. If the radiographs appear superficially normal it is important to check again and answer the following questions:
▪ Are the cortical margins of the femoral neck really smooth and continuous?
▪ Is there a black (ie lucent) line crossing the femoral neck?
▪ Does a dense white line (impaction in a compression fracture) cross the neck?
▪ Is there any angulation of the neck… compared with the uninjured side?
Approximately 1% of femoral neck fractures will be undetectable on the initial radiographs1. If the radiographs appear normal and there is strong clinical suspicion of a fracture (eg pain on weight bearing) then referral for a same day MRI, CT, or radionuclide examination is indicated. MRI is the preferred investigation.
The fracture that is most frequently missed/overlooked is an undisplaced intracapsular fracture2.


Pubic ramus fracture
A fracture of a pubic ramus can mimic the symptoms and signs of an undisplaced femoral neck fracture.
Helpful hint: following a simple fall it is rare for a patient to sustain both a femoral neck fracture and a pubic ramus fracture.


Adolescent patient with acute hip pain4,5
Apophyseal injuries (See also pp. 222–225)
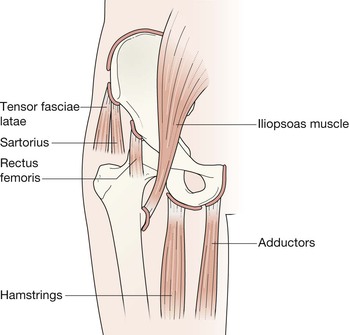
Many of the conditions presenting as acute hip pain in this age group are actually injuries to the pelvis. Always consider an apophyseal injury in a young patient.
Avulsions occur most commonly in sports where a quick burst movement or explosive action occurs. Until the growth centre fuses to the underlying bone (at any time between the ages of 16 and 25 years) an apophysis represents a site of weakness and is vulnerable to forceful muscle contraction. The sites most commonly affected are:
Always evaluate the iliac apophyses as well as the upper femoral apophyses.
Sometimes bone overgrowth/fragmentation/calcification at the injured site might be initially misinterpreted as indicating a tumour6.
Clinical impact guideline: treatment of an apophyseal injury is invariably conservative and based on rest and pain relief. Nevertheless, correct diagnosis is still important.



Uncommon but important injuries
Acetabular fracture


Dislocations7,8
These injuries result from high energy trauma.
Dislocations can be posterior, anterior, or central. Approximately 80% are posterior.
Posterior dislocation.
The extreme force is transmitted up the shaft of the femur, typically in a driver or front seat passenger involved in a road traffic accident (RTA).
The AP view usually demonstrates the dislocation very clearly. The lateral radiograph will confirm the diagnosis.
Young male (RTA).
The femoral head is dislocated posteriorly.
A large fragment has been detached from the acetabular margin and lies above the head of the femur. Several other fractures also resulted from the violent impact on this driver at the time of the collision.

Fractures of the acetabular margin are common complications of posterior dislocation.
The incidence of an accompanying acetabular fracture can be as high as 70%7. Accompanying fractures of the femoral head or neck also occur. An unrecognised acetabular fragment can prevent reduction or result in instability if the acetabular defect is large. In this patient, the dislocation has been complicated by two fragments detached from the acetabular margin. The fragments are situated superiorly and inferiorly.

Central dislocation of the head of the femur with fracture of the acetabulum.
The description “central dislocation” is common parlance for this finding. It is not a true dislocation because the femoral head remains within the socket… but it has been forced through the medial wall and lies, in part, within the pelvis.

Dislocation following total hip replacement (THR).
Easy to recognise. Occurs much more commonly following a THR for a femoral neck fracture than after an elective THR for other indications9.
Most dislocations occur in the early postoperative period. Some will dislocate later and attend the Emergency Department; some will become recurrent dislocators.


The most basic requirement.
Your ability to detect subtle fractures involving the hip and the adjacent pelvis depends upon your awareness of the normal radiological anatomy (pp. 228–229). Good understanding is essential. This radiograph is normal.
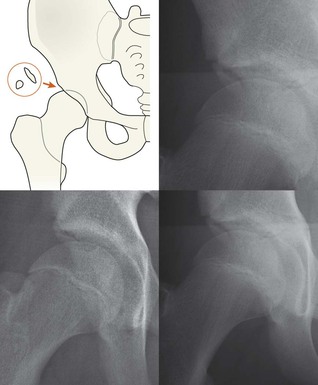
Pitfall
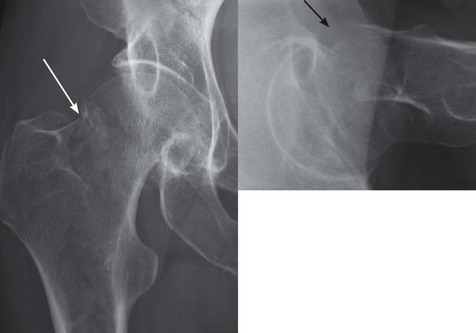
Os acetabuli.
A small bone fragment/ossicle at the superior margin of the acetabular rim is a common finding. It might represent an unfused secondary ossification centre (an os acetabuli), or a fragment due to femero-acetabular impingement10.
This ossicle/fragment is most unlikely to represent an acute fracture.
A specialist orthopaedic assessment will invariably distinguish between an unimportant ossicle (an os acetabuli) and an impingement fragment representing a longstanding injury.
See also p. 226.
[/level-membership-for-radiology-category][not-level-membership-for-radiology-category]
Hip & proximal femur
Normal anatomy
AP view
AP and lateral views
The femoral neck should:
The intertrochanteric region should:
Secondary centres (apophyses)
The femur and pelvis of an adolescent will show several small secondary centres (the apophyses).
Analysis: the checklists
Detailed inspection should focus on the specific clinical history. Thus…
An elderly patient has suffered a simple fall
Check for:
▪ A black line—a displaced fracture—across the femoral neck.
A few fractures are very difficult to detect. If the radiographs appear superficially normal it is important to check again and answer the following questions:
An adolescent patient has acute/chronic pain following athletic activity
Check that:
Patient of any age who has sustained high velocity trauma
Check all of the features described above and also check:
Hip pain in a young patient with no history of recent trauma
▪ Age 4–10 years: consider Perthe’s disease of the femoral head.
▪ Around the age of puberty: consider slipped capital femoral epiphysis.
Normal lateral view. The same patient as above. The two sites that must be checked are the neck of the femur and the trochanteric region. This peculiar projection might seem anatomically counterintuitive—see explanation on p. 228.
The common injuries
Elderly patient after a simple fall
[/not-level-membership-for-radiology-category]
