High Uterosacral Ligament Suspension With Fascial Reconstruction: Abdominal Approach
This repair is based on the concept that the uterosacral ligaments do not attenuate in cases of uterovaginal prolapse or posthysterectomy vaginal vault prolapse but instead break at certain points. The remnants of the uterosacral ligaments or the most distal ends are identified and tagged. The remnants are usually found in the vicinity of the ischial spines on each side (Fig. 42–1).
The ureters are identified on each side, and the enterocele is addressed by excision of the sac or by abdominal obliteration of the cul-de-sac. Three or four permanent sutures then are placed to plicate the ends of the uterosacral ligaments across to the midline. This creates a durable ridge to which the vaginal vault can be attached (see Fig. 42–1). A sponge stick or an EEA (end-to-end anastomosis) sizer is usually placed in the vagina, and the peritoneum over the apex of the vagina is opened. The endopelvic fascia and the muscular component or fascia of the anterior and posterior vaginal walls are identified. Nonabsorbable sutures then are used to suspend the prolapsed vagina with its fascia to the uterosacral ligaments. This is usually accomplished by placing numerous longitudinal nonabsorbable sutures through the ridge of uterosacral ligaments down the cul-de-sac, through the upper edge of the rectovaginal fascia, into the vaginal vault, and finally through the edge of the pubocervical fascia (Fig. 42–2). Tying of the sutures (see Fig. 42–2, inset) elevates the apex of the vagina to the uterosacral ligaments and creates continuity between the pubocervical fascia and the rectovaginal fascia.
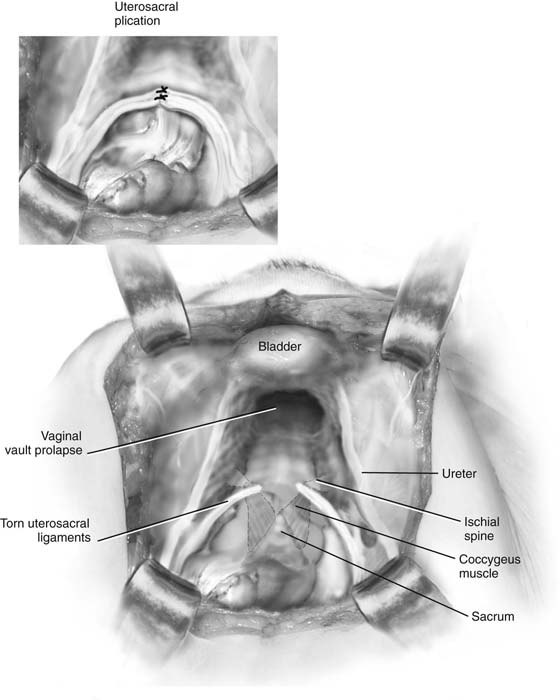
FIGURE 42–1 Abdominal view of an enterocele and vaginal vault prolapse. Note the broken ends of the uterosacral ligaments at the level of the ischial spine. The inset demonstrates plication of ligaments, creating a firm durable ridge in the hollow of the sacrum to which the vaginal vault will be suspended.
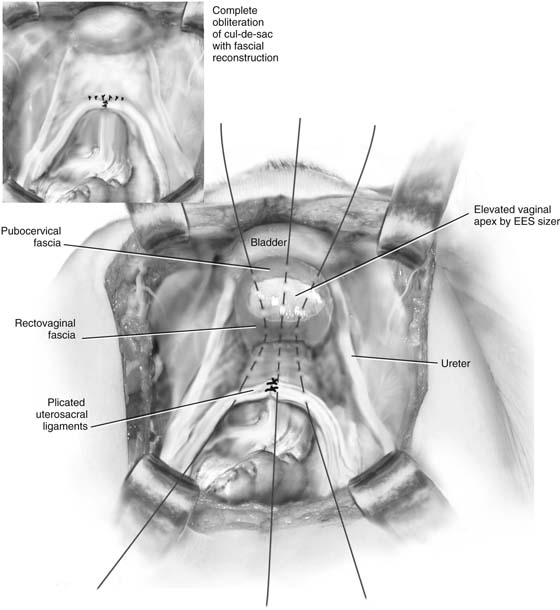
FIGURE 42–2 Longitudinally placed nonabsorbable sutures are passed through the ridge of uterosacral ligaments, down the cul-de-sac to the edge of the rectovaginal fascia, into the vaginal vault, and finally through the edge of the pubocervical fascia. Tying of the sutures (inset) elevates the apex of the vagina to the uterosacral ligaments and reapproximates the pubocervical fascia with the rectovaginal fascia.






