Section 1: Blisters (vesicles and bullae)
1
Herpes simplex infections

 Neonatal herpes. Grouped vesicles on a red base on the scalp of a 9-day-old.
Neonatal herpes. Grouped vesicles on a red base on the scalp of a 9-day-old.

 Neonatal herpes. Widespread vesicles and erosions in 2-day-old.
Neonatal herpes. Widespread vesicles and erosions in 2-day-old.

Primary herpes gingivostomatitis. Oral erosions seen in this 3-month-old.

Primary herpes gingivostomatitis. Perioral and lip vesicles in a 10-month-old infant.

Recurrent herpes labialis with grouped vesicles on upper lip.

Recurrent herpes labialis with grouped vesicles on lower lip.

Herpes keratitis. Grouped vesicles on lower eyelid and red eye in child.

Herpes facialis. Recurrent grouped vesicles on child’s cheek. No eye involvement.

Herpetic whitlow. Grouped vesicles on red base at base of thumb in thumbsucker.

Herpetic whitlow. Grouped vesicles on middle finger of child.
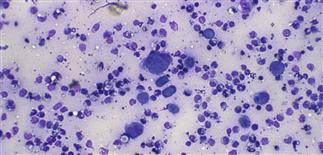
Photomicrograph of smear of blister contents showing transformed epidermal cells (giant cells) in herpes simplex infection.

Eczema herpeticum. Numerous vesicles and erosions in child with atopic dermatitis and HSV 1 infection.
CLINICAL FEATURES
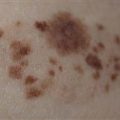
Grouped vesicles on a red base are the characteristic lesions of herpes simplex regardless of location on the skin. On mucous membrane, the blister roof is easily shed and erosions are seen. A variety of clinical patterns are seen.
Recurrent herpes simplex infection Herpes simplex viruses may persist in nerve ganglia and reactivate after UV light exposure, fever, trauma or menses. Vesicles recurring in the same site should be considered to be due to herpes simplex.
Herpes facialis Recurrent episodes of grouped vesicles on the forehead or cheek are less common and misdiagnosed.
Herpes simplex in the immunosuppressed Atypical appearances of HSV occur in the immunosuppressed, genetic immune deficiencies, children with cancer or the malnourished child. Grouped vesicles progress to giant bullae and erosions often with purpura or hemorrhage. After 24–48 hours, widespread lesions may appear. The red base may not be evident.
Eczema herpeticum (Kaposi’s varicelliform eruption) Children with atopic dermatitis may develop superinfection with HHV 1 with multiple groups of vesicles and high fever. Herpes encephalitis or pneumonia may ensue if untreated.