11 Hernias
Anatomy of the Abdominal Wall





External Oblique (EO) Muscle
• On each side, the lower border of its aponeurosis attaches to anterior superior iliac spine and pubic tubercle to form the inguinal ligament.
• Distally, a portion of EO aponeurosis fibers arch posteriorly to insert on the superior pubic ramus, forming the lacunar ligament (of Gimbernat).
• Most lateral of these deep (lacunar) fibers continue to run along the pectin of pubis as the pectineal ligament (of Cooper).
• Some of the most distal fibers arch upward, avoid the pubic tubercle, and merge with the opposite side’s fibers as the reflected inguinal ligament.
• Most muscle and aponeurotic fibers run superolateral to inferomedial (“hands in pockets” orientation).
Internal Oblique (IO) Muscle
• Fibers run deep, approximately perpendicular to the external oblique layer, from the deep lumbar aponeurosis, curving anteriorly then medially.
• Medial IO aponeurosis layer splits to pass around the rectus, as the middle layer of the rectus sheath, above the semicircular lines (of Douglas).
Transversus Abdominis (TA) Muscle
• Fibers run deep to the internal oblique layer, mostly posteriorly, becoming largely aponeurotic laterally in the deep back.
• Medial aponeurotic fibers pass posterior to the rectus, as the posterior layer of the rectus sheath, above the semicircular lines (of Douglas).
• On each side, the inferior triangle of the TA aponeurosis fuses with the internal oblique aponeurosis to form the conjoined (conjoint) tendon.
Rectus Abdominis Muscle
• Parallel segments of muscle with vertically running fibers; segments joined end-to-end by tendinous insertions (inscriptions)
• External oblique aponeurosis is always the most superficial (anterior) component of the rectus sheath.
• Internal oblique aponeurosis splits to run in front of and behind rectus in the sheath above the semilunar lines (somewhat above umbilicus).
• External and internal oblique and transversus aponeuroses components of rectus sheath pass anterior to the rectus below the semicircular lines (below the umbilicus).



Linea Alba
Transversalis Fascia
• Tough fascial layer just deep to the transversus muscle and aponeurosis, rectus sheath, and rectus abdominis anteriorly
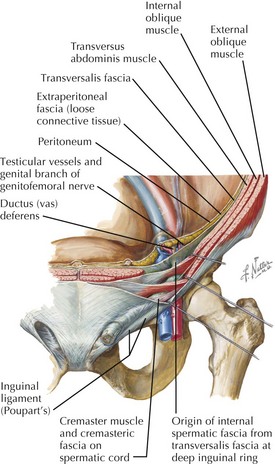
• Male transversalis fascia outpockets through the deep (internal) inguinal ring, a gap in the transversus abdominis, lateral to the inferior epigastric arteries.
• Internal spermatic fascia: transversalis fascia layer surrounding the layers of the tunica vaginalis around the descended testis, its duct, and vessels
Hesselbach’s Triangle
Inguinal Canal Boundaries





Vessels and Lymphatics
Regional Arteries and Veins
• External iliac arteries and veins run across the pelvic brim, passing under the inguinal ligament to become the femoral arteries and veins.
• Inferior epigastric vessels arise from the external iliac vessels just before they pass through the inferior abdominal wall.
• Inferior epigastric vessels run superiorly through the deep surface of the rectus abdominis, to anastomose within it with branches of superior epigastrics.
• Testicular arteries pass down from their source on the aorta (renal levels) to enter deep inguinal ring with ductus deferens and pass with spermatic cord through inguinal canal to attach to testis.
Clinical Correlates
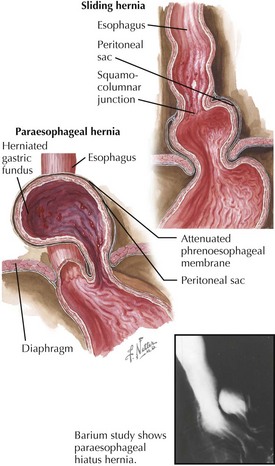
• In hernias, portions of peritoneum (sac), abdominal fat, or adjacent viscus or viscera protrude through defects or gaps in abdominal wall.
• Incarceration: abdominal contents are trapped in the hernia, can progress to strangulation (acute: emergency)
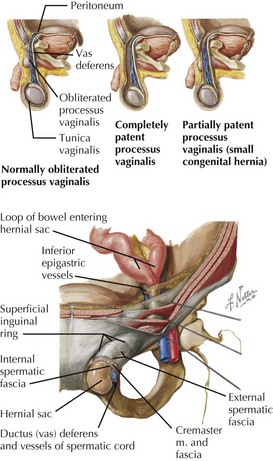
Inguinal Hernia
Types
















Umbilical Hernia
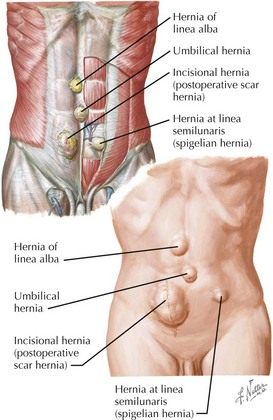
Incisional Hernia
• Causes include clinical or subclinical wound infection, poor healing, ascites, malnutrition, pregnancy, chemotherapy, steroids, strain on the wound.