[level-membership-for-radiology-category] Normal liver length 8-12 cm for men, 6-10 cm for women in midclavicular line






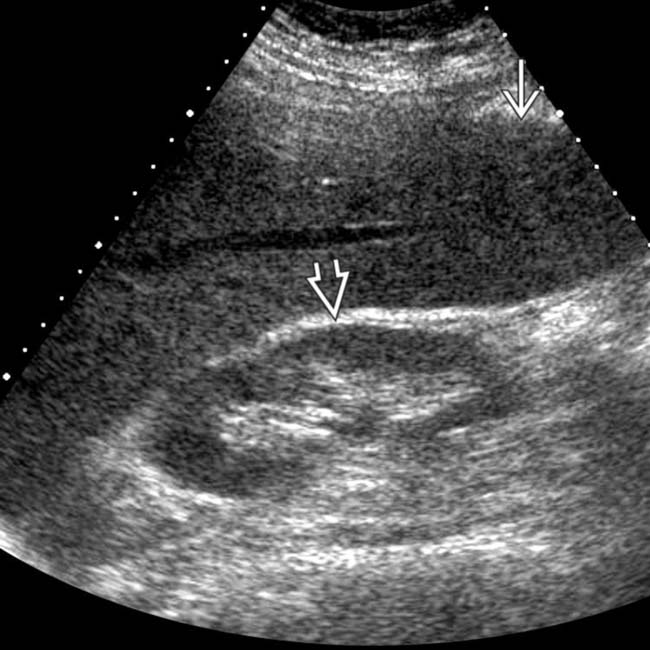
 , extending caudally below the level of the kidney
, extending caudally below the level of the kidney  .
.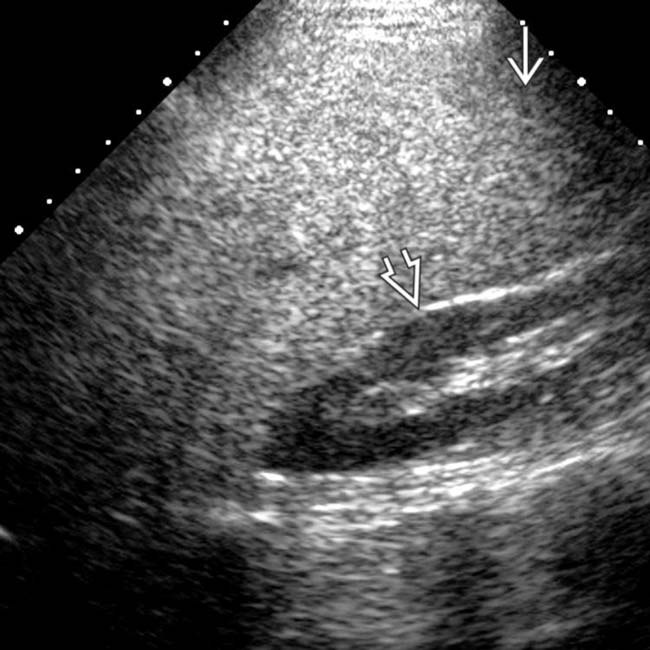
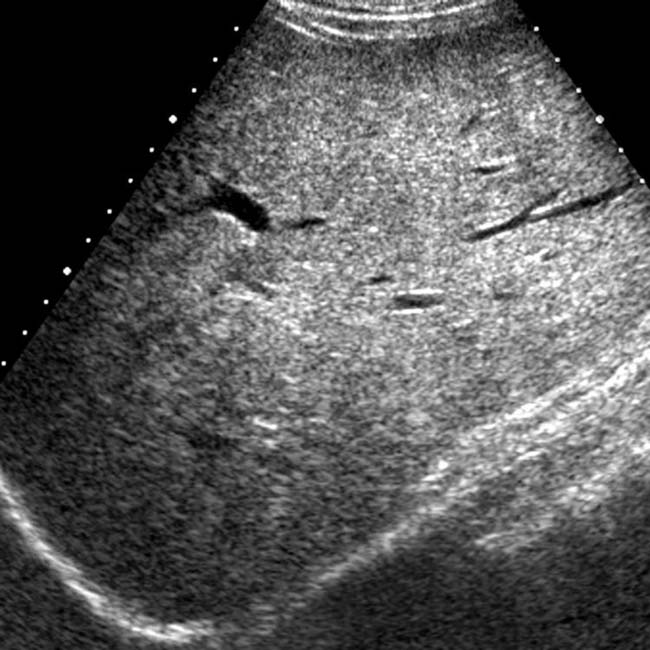
 extending below the level of the right kidney
extending below the level of the right kidney  as well as echogenicity greater than that of the kidney due to diffuse steatosis.
as well as echogenicity greater than that of the kidney due to diffuse steatosis.
 .
.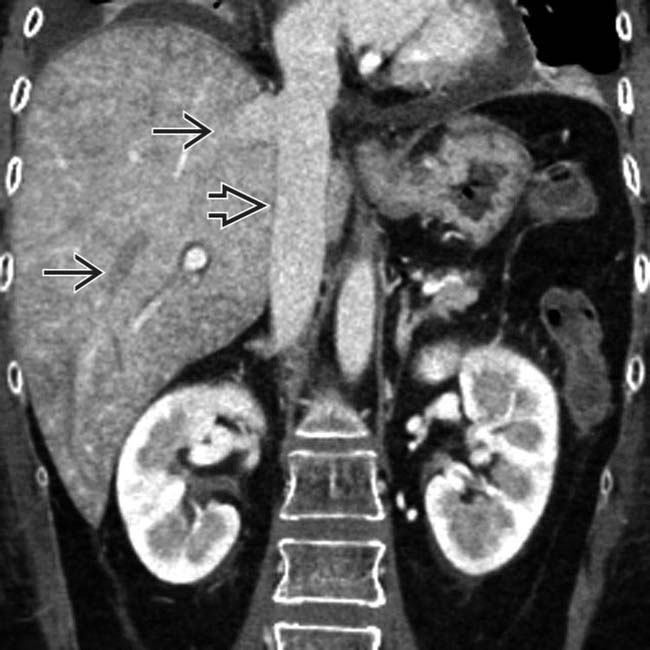
 and IVC
and IVC  due to passive congestion of the liver. Drug toxicity accounted for the cardiac dysfunction.
due to passive congestion of the liver. Drug toxicity accounted for the cardiac dysfunction.

























[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Normal liver length 8-12 cm for men, 6-10 cm for women in midclavicular line
, extending caudally below the level of the kidney . extending below the level of the right kidney as well as echogenicity greater than that of the kidney due to diffuse steatosis.. and IVC due to passive congestion of the liver. Drug toxicity accounted for the cardiac dysfunction.IMAGING
General Features
Imaging Recommendations
• Protocol advice
Buy Membership for Radiology Category to continue reading. Learn more here
[/not-level-membership-for-radiology-category]
