CHAPTER 36 Hepatic Tumors
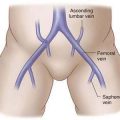
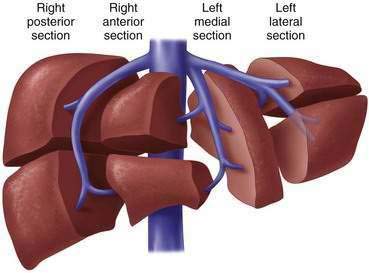
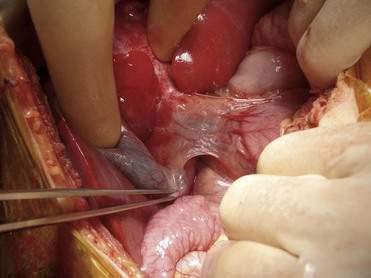
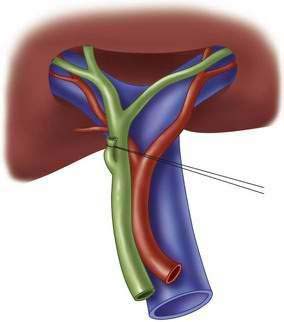
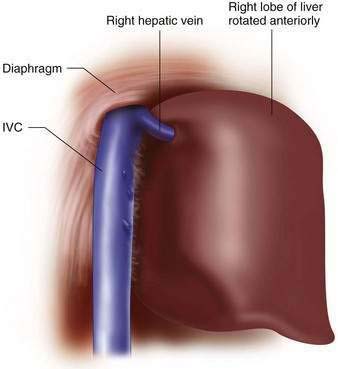
Step1: Surgical Anatomy
Step 2: Preoperative Considerations



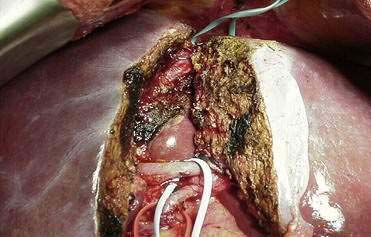
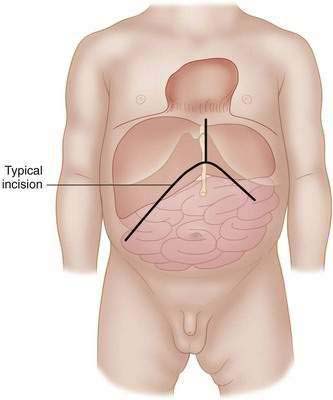
Step 3: Operative Steps

Step 4: Postoperative Care
Step 5: Pearls and Pitfalls
Cho CS, Park J, Fong Y. Hepatic resection. In: ACS surgery: Principles and practice. WebMD; 2007.
De Ville de Goyet J, Otte J-B. Liver tumors and resections. In: Stinger MD, Oldham KT, Mouriquand PDE, editors. Pediatric surgery and urology: Long-term outcomes. 2nd ed. New York: Cambridge University Press; 2006:799-814.
Giuliante F, Nuzzo G, Ardito F, et al. Extraparenchymal control of hepatic veins during mesohepatectomy. J Am Coll Surg 206:496-502.
Gonzalez RJ, Barnett CBJr. A technique for safely teaching major hepatectomy to surgical residents. Am J Surg. 2008;195:521-525.
Poon RT. Current techniques of liver transection. HPB. 2007;9:166-173.
Poon RT. Recent advances in techniques of liver resection. Surg Technol Int. 2004;13:71-77.
Vollmer CM, Dixon E, Sahajpal A, et al. Water-jet dissection for parenchymal division during hepatectomy. HPB. 2006;8:377-385.
Yao P, Morris DL. Radiofrequency ablation-assisted liver resection: review of the literature and our experience. HPB. 2006;8:248-254.