Chapter 25 Hemoptysis
1 What is hemoptysis?



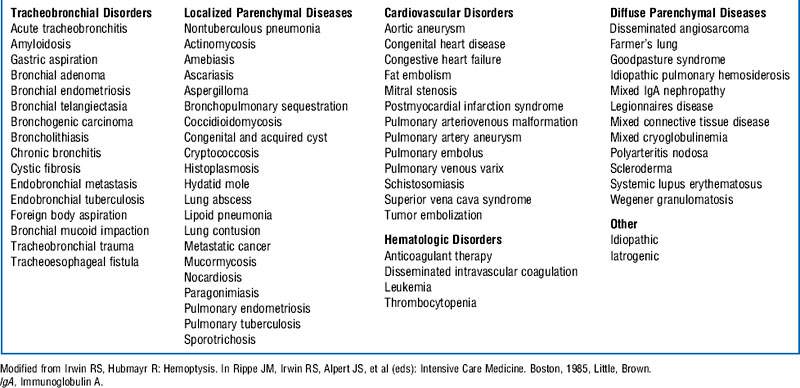
3 Describe the differential diagnosis of hemoptysis
The differential diagnosis of hemoptysis is based on the site of bleeding. Hemoptysis in general results from either a focal or a diffuse tracheobronchial (airway) or pulmonary parenchymal process (Box 25-1). Occasionally nonpulmonary processes, in particular cardiac, vascular, or hematologic disorders, may result in bleeding in the lungs. The frequency with which hemoptysis is associated with these conditions is determined by the age of the patient, the population being studied (e.g., surgical vs. medical, veterans hospital vs. city or county indigent hospital), and the amount of expectorated blood. Approximately 30% of cases are cryptogenic, and no explanation for hemoptysis is determined despite extensive evaluation.
8 What is the initial approach to the evaluation of a patient with hemoptysis in the intensive care unit?
11 Describe the immediate management of massive hemoptysis
The goals of immediate management of patients with massive hemoptysis are as follows:
12 What specific therapies may be useful to stop ongoing hemorrhage?





Controversy
18 Should fiberoptic bronchoscopy be performed before bronchial artery embolization in patients with massive hemoptysis?
 Is important in guiding bronchial artery embolization by identifying the site of bleeding
Is important in guiding bronchial artery embolization by identifying the site of bleeding

 Facilitates the use of a number of techniques that can control bleeding
Facilitates the use of a number of techniques that can control bleeding





1 Bussières J.S. Iatrogenic pulmonary artery rupture. Curr Opin Anaesthesiol. 2007;20:48–52.
2 Chun J.Y., Morgan R., Belli A.M. Radiological management of hemoptysis: a comprehensive review of diagnostic imaging and bronchial arterial embolization. Cardiovasc Intervent Radiol. 2010;33:240–250.
3 Hsiao E.I., Kirsch C.M., Kagawaa F.T., et al. Utility of fiberoptic bronchoscopy before bronchial artery embolization for massive hemoptysis. Am J Roentgenol. 2001;177:861–867.
4 Ibrahim W.H. Massive haemoptysis: the definition should be revised. Eur Respir J. 2008;32:1131–1132.
5 Jean-Baptiste E. Clinical assessment and management of massive hemoptysis. Crit Care Med. 2000;28:1642–1647.
6 Johnson J.L. Manifestations of hemoptysis: how to manage minor, moderate, and massive bleeding. Postgrad Med. 2002;112:101–113.
7 Jougon J., Ballester M., Delcambre F., et al. Massive hemoptysis: what place for medical and surgical treatment. Eur J Cardiothorac Surg. 2002;22:345–351.
8 Kalva S.P. Bronchial artery embolization. Tech Vasc Interv Radiol. 2009;12:130–138.
9 Lordan J.L., Gascoigne A., Corris P.A. The pulmonary physician in critical care: illustrative case 7: assessment and management of massive haemoptysis. Thorax. 2003;58:814–819.
10 Menchini L., Remy-Jardin M., Faivre J.B., et al. Cryptogenic haemoptysis in smokers: angiography and results of embolisation in 35 patients. Eur Respir J. 2009;34:1031–1039.
11 Praveen C.V., Martin A. A rare case of fatal haemorrhage after tracheostomy. Ann R Coll Surg Engl. 2007;89(8):1–3.
12 Sakr L., Dutau H. Massive hemoptysis: an update on the role of bronchoscopy in diagnosis and management. Respiration. 2010;80:38–58.
13 Savale L., Parrot A., Khalil A., et al. Cryptogenic hemoptysis: from a benign to a life-threatening pathologic vascular condition. Am J Respir Crit Care Med. 2007;175:1181–1185.
14 Shigemura N., Wan I.Y., Yu S.C., et al. Multidisciplinary management of life-threatening massive hemoptysis: a 10-year experience. Ann Thorac Surg. 2009;87:849–853.
15 Valipour A., Kreuzer A., Koller H., et al. Bronchoscopy-guided topical hemostatic tamponade therapy for the management of life-threatening hemoptysis. Chest. 2005;127:2113–2118.
16 Wang G.R., Ensor J.E., Gupta S., et al. Bronchial artery embolization for the management of hemoptysis in oncology patients: utility and prognostic factors. Vasc Interv Radiol. 2009;20:722–729.
17 Yoon W., Kim J.K., Kim Y.H., et al. Bronchial and nonbronchial systemic artery embolization for lifethreatening hemoptysis: a comprehensive review. Radiographics. 2002;22:1395–1409.
