CHAPTER 3 Heller myotomy with toupet or dor fundoplication for achalasia
Step 1. Clinical anatomy
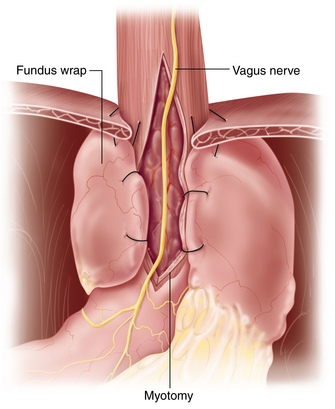
♦ The sling fibers of Willis on the cardia of the stomach provide some competency of the lower esophageal sphincter (LES). Therefore, to completely obliterate these fibers, the myotomy should be carried at least 3 cm onto the stomach.
♦ To ensure an adequate myotomy onto the stomach, both the cardioesophageal fat pad and anterior (left) vagus should be mobilized as they cover the portion of cardia that is included in the myotomy.
♦ In patients with end-stage achalasia and a dilated sigmoid esophagus, the gastroesophageal (GE) junction is often angulated. Therefore, consideration for not doing a fundoplication should be given lest the distal esophagus be angulated more.
Step 2. Preoperative considerations
♦ Manometry is essential to make the diagnosis, demonstrating an aperistaltic esophagus and an incomplete relaxation of the LES.
♦ Upper endoscopy and fluoroscopic evaluation should be used to exclude other pathology and to determine the amount of esophageal dilation.
♦ In patients over 50 years of age, symptoms less than 6 months, or those with significant weight loss (>10 to 20 lbs), CT scan or endoscopic ultrasound should be performed to rule out pseudoachalasia (i.e., a tumor obstructing the esophagus).
♦ In patients with atypical presentations, botulinum toxin A (Botox) can be used as a diagnostic tool to identify those who would benefit from a myotomy.
Positioning
♦ Patients are placed in modified lithotomy with both arms tucked.
♦ A beanbag overhangs the edge of the operative table to form a saddle around the patient’s perineum to avoid sliding.
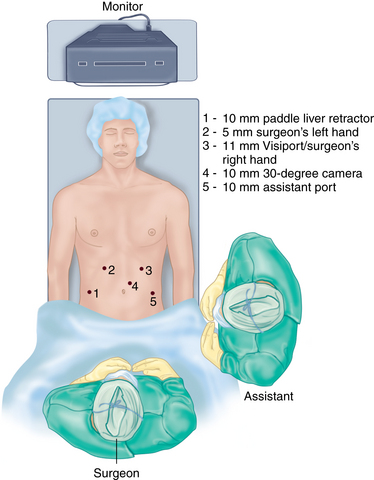
♦ The operative surgeon stands between the patient’s legs with the assistant at the patient’s left side.
♦ Monitors are placed above the patient’s head.
♦ An oral-gastric tube can be used to decompress the stomach and then removed.
♦ After port placement, the patient is placed in steep reverse Trendelenburg position.
Step 3. Operative steps
Port placement
♦ A small incision is made at the left costal margin in the mid-clavicular line.
♦ Pneumoperitoneum is established using a Veress needle, and the abdomen is entered using a Visiport trocar (Covidien; Mansfield, Massachusetts).
♦ The camera port is placed 4 cm left of midline and one hand’s breadth (approximately 10-12 cm) inferior to the left costal margin.
♦ A 10-mm 30-degree laparoscope camera provides superior visualization.
♦ The remaining four ports are placed under direct visualization.
♦ A 5-mm trocar is placed in the right upper quadrant (surgeon’s left hand), a 10-mm trocar is placed in the right lateral quadrant (paddle liver retractor), and 10-mm trocar is placed in the left lower quadrant (assistant port) (Figure 3-1).
Mobilization of esophagus
♦ The left phrenogastric ligament is divided to expose the left crus.
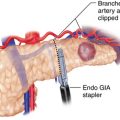
♦ The gastric fundus is mobilized by dividing the short gastric vessels using an ultrasonic dissector.
♦ Posterior attachments between the proximal stomach and retroperitoneum are divided to minimize tension on the subsequent fundoplication.
♦ The left phrenoesophageal membrane is divided.
♦ The gastrohepatic ligament is divided and carried toward the esophageal hiatus to expose the right crus.
♦ The nerves of Latarjet and aberrant or accessory vessels are preserved.
♦ The anterior phrenoesophageal membrane is divided.
♦ The anterior (left) vagus is identified, protected, and separated from the esophagus.
♦ A posterior esophageal window is created, which exposes the confluence of the right and left crus.
♦ The posterior (right) vagus is visualized and protected.
♦ A Penrose drain can be placed around the GE junction to retract the esophagus during the mobilization.
♦ An extensive hiatal and mediastinal esophageal dissection is performed to maximize the length of the myotomy.
♦ The cardioesophageal fat pad attachments to the underlying stomach and esophagus are divided. In doing so, the anterior (left) vagus is preserved and separated from the GE junction.
♦ This fat pad to the left of the anterior (left) vagus is then resected.
Myotomy
♦ A lighted 50 F bougie is passed into the body of the stomach.
♦ A Babcock retractor is draped over the bougie, just distal to the GE junction, gently stretching the muscle fibers.
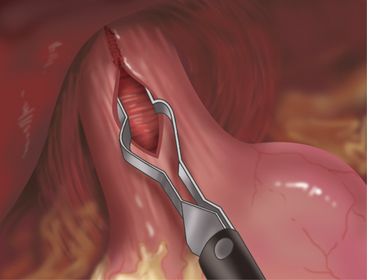
♦ The myotomy is performed with an L-shaped hook electrocautery device, starting on the anterior surface at the 10 o’clock position. Individual muscle fibers divide easily under gentle traction, rarely utilizing cautery.
♦ The longitudinal muscle fibers are divided first, exposing the inner circular muscle of the esophagus (sling fibers of Willis on the cardia). Submucosal bleeding should be controlled with pressure, not cautery (Figure 3-2).
♦ The myotomy should be extended as proximal as possible (6 to 8 cm) and at least 3 cm onto the cardia of the stomach.
Toupet fundoplication
♦ The posterior gastric fundus is brought around the esophagus and secured to the right crus and to the right edge of the myotomy.
♦ The posterior fundus is further secured to the right by suturing it to the base of the right crus.
♦ A row of two or three sutures is used to attach the posterior fundus to the right side of the esophagus near the myotomy.
♦ In a similar fashion the anterior fundus is secured to the left crus and left edge of the myotomy.
♦ The hiatus is not closed, unless a large hernia is encountered.
♦ Upper endoscopy is performed to exclude mucosal injury during the myotomy and to ensure no resistance or angulation of the fundoplication (Figure 3-3).
Dor fundoplication
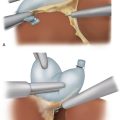
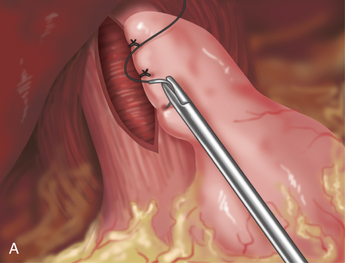
♦ This fundoplication folds the anterior fundus over the anterior esophagus to form an anterior flap and to re-create the angle of His. Two vertical rows of sutures are placed, one to the left (performed first) and one to the right side of the esophagus.
♦ The uppermost stitch incorporates the anterior gastric fundus to the left crus and left edge of the myotomy.
♦ The remaining two sutures are used to attach the anterior fundus to the left side of the esophagus near the myotomy, thus completing the first vertical row (Figure 3-4a).
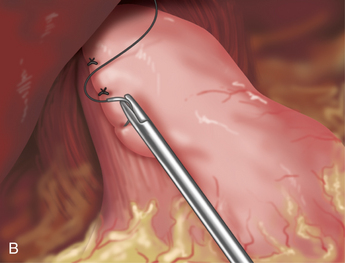
♦ The gastric fundus is then folded over the esophagus from left to right to cover the myotomy.
♦ The greater curve of the fundus is secured to the right crus and to the right edge of the myotomy (Figure 3-4b).
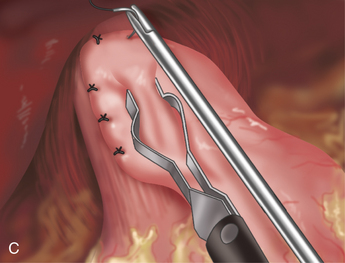
♦ In a similar fashion, the remaining two sutures secure the fundus to the right side of the esophagus near the myotomy.
♦ One or two final sutures are used to secure the fundus to the anterior hiatus to prevent the fundus from angulating the esophagus at the GE junction (Figure 3-4c).
♦ Upper endoscopy is performed to exclude mucosal injury during the myotomy and to ensure no resistance or angulation of the fundoplication.
Step 4. Postoperative care
♦ Patients generally start liquids the night of their procedure.
♦ Nausea is aggressively treated with antiemetics.
♦ Average length of stay is 1 to 2 days.
♦ All medications are in liquid form for 3 to 4 weeks.
♦ Patients are slowly progressed from liquids to solid foods.
♦ Resumption of normal diet and activities occurs within 3 to 4 weeks.
♦ Manometry and 24-hour pH studies are performed 6 months after surgery to rule out asymptomatic but pathologic gastroesophageal reflux disease, which is present in 15% to 20% of patients.
Step 5. Pearls and pitfalls
♦ The lighted bougie serves to illuminate the esophagus, shows the muscle layers to be divided, and provides a stable platform on which to perform the myotomy.
♦ Minimal cautery use during the myotomy prevents delayed perforations resulting from thermal mucosal injury.
♦ Intraoperative mucosal perforations can be repaired primarily with fine (4-0 or 5-0) absorbable suture with little or no morbidity.
♦ If a mucosal laceration should occur, perform a Dor fundoplication, which serves to buttress the repaired mucosa, minimizing subsequent leaks or fistulas.
♦ There are no data to substantiate the superiority of either Toupet or Dor fundoplication in combination with a Heller myotomy for achalasia. They each have their purported benefits. The Toupet is thought to be a better antireflux procedure and may keep the myotomy tented open. The Dor does not require taking down the short gastric vessels and can buttress the mucosa as described here.
Richards WO, Torquati A, Holzman MD, et al. Heller myotomy versus Heller myotomy with Dor fundoplication for achalasia: a prospective randomized double-blind clinical trial. Ann Surg. 2004;240;3:405-412.
Woltman TA, Oelschlager BK, Pellegrini CA. Achalasia. Surg Clin North Am. 2005;85(3):483-493.
Wright AS, Williams CW, Pellegrini CA, et al. Long-term outcomes confirm the superior efficacy of extended Heller myotomy with Toupet fundoplication for achalasia. Surg Endosc. 2007;21(5):713-718.