Chapter 23
Heart Failure Evaluation and Long-Term Management
Arunima Misra, MD, FACC, Kumudha Ramasubbu, MD, FACC, Shawn T. Ragbir, MD, Glenn N. Levine, MD, FACC, FAHA and Biykem Bozkurt, MD, PhD, FACC, FAHA
This chapter deals specifically with the evaluation and long-term management of patients with heart failure caused by depressed ejection fraction. The management of patients with heart failure with preserved ejection fraction (diastolic dysfunction) is discussed in Chapter 24. The management of patients with acute decompensated heart failure is discussed in Chapter 22. Specific discussions of the evaluation and management of myocarditis, dilated cardiomyopathy, hypertrophic cardiomyopathy, and restrictive/infiltrative cardiomyopathy, as well as consideration with cardiac transplantation, are discussed in other dedicated chapters in this section of the book. The roles of pacemakers and implantable cardioverter-defibrillators in patients with heart failure are discussed in this chapter, as well as in the chapters on pacemakers (Chapter 37) and implantable cardioverter-defibrillators (Chapter 38).
1. What are the most common causes of heart failure?
2. What elements should the initial assessment of the patient with heart failure include?
Initial assessment of the patient with heart failure should include:
 Evaluation of heart failure symptoms and functional capacity (dyspnea on exertion, orthopnea, paroxysmal nocturnal dyspnea [PND], fatigue, and lower extremity edema)
Evaluation of heart failure symptoms and functional capacity (dyspnea on exertion, orthopnea, paroxysmal nocturnal dyspnea [PND], fatigue, and lower extremity edema)


 Laboratory tests, including complete blood cell count (CBC), creatinine and blood urea nitrogen (BUN), serum electrolytes, natriuretic peptide (BNP or NT-proBNP), fasting blood glucose, lipid profile, liver function tests, thyroid-stimulating hormone (TSH), and urine analysis; and screening for hemochromatosis and human immunodeficiency virus (HIV), pheochromocytoma, amyloidosis, or rheumatologic diseases reasonable in selected patients, particularly if there is clinical suspicion for testing
Laboratory tests, including complete blood cell count (CBC), creatinine and blood urea nitrogen (BUN), serum electrolytes, natriuretic peptide (BNP or NT-proBNP), fasting blood glucose, lipid profile, liver function tests, thyroid-stimulating hormone (TSH), and urine analysis; and screening for hemochromatosis and human immunodeficiency virus (HIV), pheochromocytoma, amyloidosis, or rheumatologic diseases reasonable in selected patients, particularly if there is clinical suspicion for testing






3. How are heart failure symptoms classified?
 Class I: No limitation; ordinary physical activity does not cause excess fatigue, shortness of breath, or palpitations.
Class I: No limitation; ordinary physical activity does not cause excess fatigue, shortness of breath, or palpitations.

 Class III: Marked limitation of physical activity; ordinary activity will lead to symptoms.
Class III: Marked limitation of physical activity; ordinary activity will lead to symptoms.

4. What is the stage system for classifying heart failure?
In 2001, the American College of Cardiology/American Heart Association (ACC/AHA) introduced a system to categorize the stages of heart failure. This system is somewhat different in focus than the previous NYHA classification system and was intended, in part, to emphasize the prevention of the development of symptomatic heart failure. In addition, the 2009 update on the 2005 Heart Failure Guidelines suggest appropriate therapy for each stage (Figure 23-1).
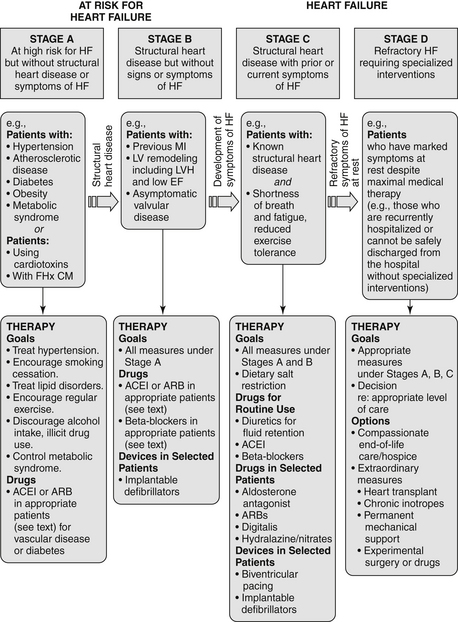
Figure 23-1 American College of Cardiology/American Heart Association Stages in the Development of Heart Failure/Recommended Therapy by Stage. (From Jessup M, Abraham WT, Casey DE, et al: ACC/AHA 2009 focused update: ACCF/AHA guidelines for the diagnosis and management of heart failure in adults : a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: Developed in collaboration with the International Society for Heart and Lung Transplantation, Circulation 119:1977-2016, 2009; originally published online March 26, 2009.) ACEI, Angiotensin-converting enzyme inhibitor; ARB, angiotensin II receptor blocker; EF, ejection fraction; FHx CM, family history of cardiomyopathy; HF, heart failure; LV, left ventricle; LVH, left ventricular hypertrophy; MI, myocardial infarction.
 Stage A: Patient is at high risk for developing heart failure but is without structural heart disease or symptoms of heart failure. Includes patients with hypertension, coronary artery disease (CAD), obesity, diabetes, history of drug or alcohol abuse, history of rheumatic fever, family history of cardiomyopathy, or treatment with cardiotoxins
Stage A: Patient is at high risk for developing heart failure but is without structural heart disease or symptoms of heart failure. Includes patients with hypertension, coronary artery disease (CAD), obesity, diabetes, history of drug or alcohol abuse, history of rheumatic fever, family history of cardiomyopathy, or treatment with cardiotoxins

 Stage C: Patient with structural heart disease and with prior or current symptoms of heart failure
Stage C: Patient with structural heart disease and with prior or current symptoms of heart failure
 Stage D: Patient with refractory heart failure requiring specialized interventions
Stage D: Patient with refractory heart failure requiring specialized interventions
5. Which patients with heart failure should be considered for endomyocardial biopsy (EMB)?
In 2007, the ACC/AHA/European College of Cardiology (ACC/AHA/ECC) issued a scientific statement on the role of EMB. Most patients who are seen for heart failure should not be referred for EMB. Biopsy results are often nonspecific or unrevealing, and in most cases there is no specific therapy based on biopsy results that have been shown to improve prognosis. However, in certain clinical scenarios, EMB should be performed (class I recommendation) or can be considered and is considered reasonable (class IIa recommendation). As given in that document, these scenarios include the following:
 New-onset heart failure of less than 2 weeks duration associated with a normal-sized or dilated left ventricle and hemodynamic compromise (class I; level of evidence B)
New-onset heart failure of less than 2 weeks duration associated with a normal-sized or dilated left ventricle and hemodynamic compromise (class I; level of evidence B)



 Heart failure associated with suspected anthracycline cardiomyopathy (class Ia; level of evidence C)
Heart failure associated with suspected anthracycline cardiomyopathy (class Ia; level of evidence C)
 Heart failure with unexplained restrictive cardiomyopathy (class IIa; level of evidence C)
Heart failure with unexplained restrictive cardiomyopathy (class IIa; level of evidence C)
6. What are the general treatments for patients with heart failure?
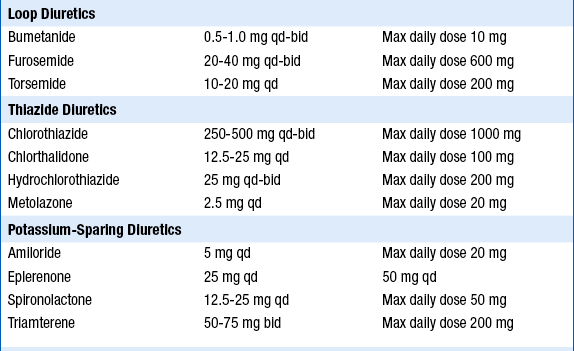
 Diuretics are indicated for volume overload. Starting doses of furosemide are often 20 to 40 mg once or twice a day, but higher doses will be required in patients with significant renal dysfunction. The dose should be uptitrated to a maximum of up to 600 mg daily in divided doses. Failure of therapy is often the result of inadequate diuretic dosing. Torsemide is more expensive than furosemide but has superior absorption and longer duration of action. Bumetanide is approximately 40 times more potent milligram-for-milligram than furosemide and can also be used in patients who are unresponsive or poorly responsive to furosemide. Synergistic diuretics that act on the distal portion of the tubule (thiazides such as metolazone, or potassium-sparing agents) are often added in those who fail to respond to high-dose loop diuretics alone. In addition, a new recommendation from 2009 Focused Update states that for hospitalized heart failure patients, if diuresis is inadequate to relieve congestion, higher doses of loop diuretics should be used, addition of second diuretic should be made or continuous infusion of a loop diuretic should be considered.
Diuretics are indicated for volume overload. Starting doses of furosemide are often 20 to 40 mg once or twice a day, but higher doses will be required in patients with significant renal dysfunction. The dose should be uptitrated to a maximum of up to 600 mg daily in divided doses. Failure of therapy is often the result of inadequate diuretic dosing. Torsemide is more expensive than furosemide but has superior absorption and longer duration of action. Bumetanide is approximately 40 times more potent milligram-for-milligram than furosemide and can also be used in patients who are unresponsive or poorly responsive to furosemide. Synergistic diuretics that act on the distal portion of the tubule (thiazides such as metolazone, or potassium-sparing agents) are often added in those who fail to respond to high-dose loop diuretics alone. In addition, a new recommendation from 2009 Focused Update states that for hospitalized heart failure patients, if diuresis is inadequate to relieve congestion, higher doses of loop diuretics should be used, addition of second diuretic should be made or continuous infusion of a loop diuretic should be considered.





The elements of long-term management of patients with CHF resulting from depressed LV systolic function are summarized in Table 23-1.
TABLE 23-1
ELEMENTS OF THE LONG-TERM MANAGEMENT OF PATIENTS WITH CONGESTIVE HEART FAILURE DUE TO LEFT VENTRICULAR SYSTOLIC DYSFUNCTION
| Treatment/Intervention | Recommendation (Level of Evidence) |
| Diuretics for fluid retention | Class I (LOE: C) |
| Salt restriction | Class I (LOE: C) |
| ACE inhibitors (ACEIs) | Class I (LOE: A) |
| Angiotensin II receptor blockers (ARB) in ACEI-intolerant patients | Class I (LOE: A) |
| ARB in persistently symptomatic patients with reduced LVEF already being treated with conventional therapy | Class IIb (LOE: C) |
| Hydralazine + Isosorbide in patients ACEI and ARB intolerant | Class IIb (LOE: C) |
| Hydralazine + Isosorbide in patients already on ACEI and β-blocker with persistent symptoms | Class IIa (LOE: A) |
| β-Blockers | Class I (LOE: A) |
| Digoxin in patients with heart failure symptoms. Generally used in those with continued symptoms and/or hospitalizations despite good therapy with diuretics and ACEIs | Class IIa (LOE: B) |
| Aldosterone antagonists in patients with moderate-severe symptoms who can carefully be monitored for renal function and potassium level and with baseline creatinine < 2-2.5 mg/dL and potassium < 5.0 mEq/L | Class I (LOE: B) |
| Exercise training in ambulatory patients | Class I (LOE: B) |
| ICD for “secondary prevention” (history of cardiac arrest, ventricular fibrillation, or hemodynamically destabilizing ventricular tachycardia) | Class I (LOE: A) |
| ICD for “primary prevention” for LVEF < 30%-35% and symptomatic heart failure (see text) | Class I-IIa (LOE: A-B) |
| Cardiac resynchronization therapy for patients in sinus rhythm with class III-IV symptoms despite medical therapy, LVEF < 35%, and QRS > 120 ms (see text) | Class I (LOE: A) |
Modified from Hunt SA, Abraham WT, Chin MH, et al: ACC/AHA 2005 guideline update for the diagnosis and management of chronic heart failure in the adult: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure). J Am Coll Cardiol 46:e1-e82, 2005.
7. How do ACE inhibitors and ARBs work?
ARBs selectively block the binding of angiotensin II to the AT1 receptor, thereby blocking the effect of angiotensin II on end organs. This results in attenuation of sympathetic tone, decrease in arterial vasoconstriction, and attenuation of myocardial hypertrophy. Because angiotensin II stimulates aldosterone production, circulating levels of aldosterone are reduced. This results in a decrease in sodium chloride absorption, potassium excretion in the distal tubules, and water retention.
8. What approach should be taken if a patient treated with an ACE inhibitor develops a cough?
9. What is the efficacy of ARBs compared with ACE inhibitors in patients with chronic heart failure?
10. When should ARBs be added to ACE inhibitors in patients with chronic heart failure?
 Continue to have symptoms of heart failure despite receiving target doses of ACE inhibitors and β-blockers
Continue to have symptoms of heart failure despite receiving target doses of ACE inhibitors and β-blockers

11. How do aldosterone antagonists work?
12. List the indications and recommended dosing of aldosterone antagonists in heart failure.
Current indications include the following:
 Chronic NYHA class III-IV heart failure and left ventricular ejection fraction 35% or less; already receiving standard therapy for heart failure, including ACE inhibitors, β-blockers, and diuretics (based on the RALES trial with spironolactone [Aldactone]). The recent EMPHASIS trial with eplerenone demonstrated improvement in survival and heart failure hospitalizations in patients with mild (NYHA class II) heart failure symptoms and systolic heart failure suggesting a wider class of patients (NYHA class II-IV) may benefit from aldosterone antagonism.
Chronic NYHA class III-IV heart failure and left ventricular ejection fraction 35% or less; already receiving standard therapy for heart failure, including ACE inhibitors, β-blockers, and diuretics (based on the RALES trial with spironolactone [Aldactone]). The recent EMPHASIS trial with eplerenone demonstrated improvement in survival and heart failure hospitalizations in patients with mild (NYHA class II) heart failure symptoms and systolic heart failure suggesting a wider class of patients (NYHA class II-IV) may benefit from aldosterone antagonism.



The initial and target doses for aldosterone antagonists and other drugs used to treat patients depressed systolic ejection fraction and/or CHF are listed in Table 23-2.
TABLE 23-2
INITIAL AND TARGET DOSES FOR COMMONLY USED DRUGS FOR PATIENTS WITH DEPRESSED SYSTOLIC EJECTION FRACTION AND/OR CONGESTIVE HEART FAILURE
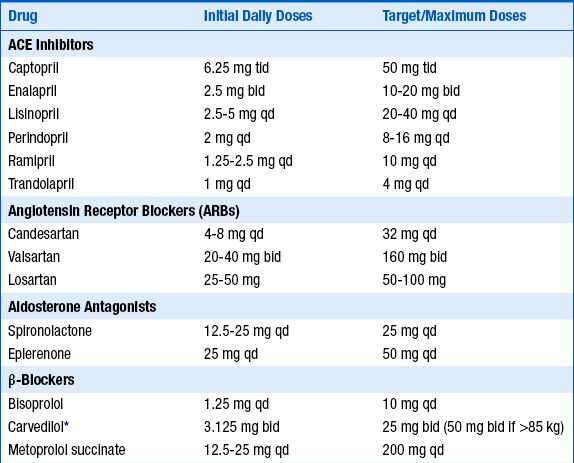
ACE, Angiotensin-converting enzyme; bid, twice a day; qd, one a day; tid three times a day.
∗Extended-release carvedilol now available, although this preparation not specifically tested in heart failure.
Modified from Hunt SA, Abraham WT, Chin MH, et al: ACC/AHA 2005 guideline update for the diagnosis and management of chronic heart failure in the adult: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure). J Am Coll Cardiol 46:e1-e82, 2005.
13. Can all patients with heart failure safely be started on an aldosterone antagonist?
14. Describe common adverse effects of ACE inhibitors, ARBs, and aldosterone antagonists.
Common adverse effects include the following:
 ACE inhibitors: hypotension, worsening renal function, hyperkalemia, cough, angioedema
ACE inhibitors: hypotension, worsening renal function, hyperkalemia, cough, angioedema


15. What are the indications and dosing of nitrates/hydralazine in patients with chronic heart failure?
Taking all the evidence together, the I/H combination is indicated in the following patients:
 Those who cannot take an ACE inhibitor or ARB because of renal insufficiency or hyperkalemia
Those who cannot take an ACE inhibitor or ARB because of renal insufficiency or hyperkalemia
 Those who are hypertensive and/or symptomatic despite taking ACE inhibitor, ARB, and β-blockers
Those who are hypertensive and/or symptomatic despite taking ACE inhibitor, ARB, and β-blockers



16. How should patients be treated with β-blockers?
 Patients should not be initiated on β-blocker therapy during decompensated or hemodynamically unstable state heart failure.
Patients should not be initiated on β-blocker therapy during decompensated or hemodynamically unstable state heart failure.

 β-Blockers should be initiated at low doses, uptitrated gradually (in at least 2-week intervals), and titrated to target doses shown to be effective in clinical trials (see Table 23-2). Practitioners should aim to achieve target doses in 8 to 12 weeks from initiation of therapy and to maintain patients at maximal tolerated doses.
β-Blockers should be initiated at low doses, uptitrated gradually (in at least 2-week intervals), and titrated to target doses shown to be effective in clinical trials (see Table 23-2). Practitioners should aim to achieve target doses in 8 to 12 weeks from initiation of therapy and to maintain patients at maximal tolerated doses.



17. What is the mechanism of action of digoxin?
18. Is there scientific evidence for the use of digoxin?
The Digitalis Investigation Group (DIG) trial was a multicenter, randomized, double-blinded, placebo-controlled study of 6801 symptomatic patients with heart failure and ejection fraction less than 45%, who were in sinus rhythm. Mean follow-up was 37 months. Patients already receiving digoxin were allowed into the trial and randomized to digoxin or placebo without a washout period. About 95% of patients in both groups received ACE inhibitors; β-blockers were not in use for heart failure at the time. The primary outcome was total mortality. Digoxin did not improve total mortality (34.8% versus 35.1% in the placebo group, P = 0.80) or deaths from cardiovascular causes (29.9% versus 29.5%, P = 0.78). Hospitalizations as a result of worsening heart failure (a secondary endpoint) were significantly reduced by digoxin (26.8% versus 34.7% in the placebo group, risk ratio 0.72, P < 0.001). Hospitalizations for suspected digoxin toxicity were higher in the digoxin group (2% versus 0.9%, P < 0.001). In an ancillary, parallel trial in patients with ejection fraction greater than 45% and sinus rhythm, the findings were consistent with the results of the main trial. Whether these results hold with contemporary heart failure treatment that includes β-blockers, aldosterone-receptor blockers, and resynchronization therapy is not known.
19. What are some of the relevant drug interactions of digoxin?
 Quinidine, verapamil, amiodarone, propafenone, and quinine (used for muscle cramps) may double digoxin levels, and the dose of digoxin should be halved when used in combination with any of these drugs.
Quinidine, verapamil, amiodarone, propafenone, and quinine (used for muscle cramps) may double digoxin levels, and the dose of digoxin should be halved when used in combination with any of these drugs.

 Thyroxine and albuterol increase the volume of distribution, resulting in decreased digoxin levels.
Thyroxine and albuterol increase the volume of distribution, resulting in decreased digoxin levels.

20. What are the clinical manifestations of digoxin toxicity?
21. What are the electrocardiographic findings of digoxin toxicity?


 First- and second-degree AV block
First- and second-degree AV block

 Paroxysmal atrial tachycardia with AV block (common)
Paroxysmal atrial tachycardia with AV block (common)
 Bidirectional ventricular tachycardia (rare but typical)
Bidirectional ventricular tachycardia (rare but typical)


 Regularized atrial fibrillation or atrial fibrillation with slow ventricular response (common)
Regularized atrial fibrillation or atrial fibrillation with slow ventricular response (common)
22. How is digoxin toxicity treated?
It depends on the clinical severity. Digoxin withdrawal is sufficient with only suggestive symptoms. Activated charcoal may enhance the gastrointestinal (GI) clearance of digoxin if given within 6 hours of ingestion. Drugs that increase plasma digoxin levels (see Question 19) should be discontinued (except amiodarone, because of its long half-life). Correction of hypokalemia is vital (intravenous [IV] replacement through a large vein is preferred with life-threatening arrhythmias), but judgment is needed in the presence of high degrees of AV block. Symptomatic AV block may respond to atropine or to phenytoin (100 mg IV every 5 minutes up to 1000 mg until response or side effects); if no response, use digoxin immune Fab (ovine) (Digibind). The use of temporary transvenous pacing should be avoided. Patients with severe bradycardia should be given Digibind, even if they respond to atropine. Lidocaine and phenytoin may be used to treat ventricular arrhythmias, but for potentially life-threatening bradyarrhythmias or tachyarrhythmias, Digibind should be used. IV magnesium may be given 2 grams over 5 minutes and has been shown to help with digoxin toxicity related arrhythmias. Dialysis has no role because of the high tissue-binding of digoxin.
23. What are the indications for Digibind?
24. What three classes of drugs exacerbate the syndrome of CHF and should be avoided in most CHF patients?
a. Antiarrhythmic agents. They can exert cardiodepressant and proarrhythmic effects. Only amiodarone and dofetilide have been shown not to adversely affect survival.
b. Calcium channel blockers. The nondihydropyridines can lead to worsening heart failure and have been associated with an increased risk of cardiovascular events. Only the dihydropyridines or vasoselective calcium channel blockers have been shown not to adversely affect survival.
c. NSAIDs. According to the ACC/AHA guidelines, nonsteroidal antiinflammatory drugs (NSAIDs) can cause sodium retention and peripheral vasoconstriction and can attenuate the efficacy and enhance the toxicity of diuretics and ACE inhibitors. The European Society of Cardiology also cautions against the use of NSAIDs.
25. Is dietary restriction of sodium recommended in patients with symptomatic heart failure?
26. Is fluid restriction recommended in all patients with heart failure?
27. Should patients with CHF be told to use salt substitutes instead of salt?
28. What are the current criteria for consideration of CRT with biventricular pacing?

 Class III or ambulatory class IV symptoms despite good medical therapy
Class III or ambulatory class IV symptoms despite good medical therapy
 LVEF less than or equal to 35%
LVEF less than or equal to 35%
 QRS more than 120 ms (especially if left bundle branch block morphology present)
QRS more than 120 ms (especially if left bundle branch block morphology present)
29. Which patients with heart failure should be considered for an ICD?
 Secondary prevention (cardiac arrest survivors of ventricular tachycardia/ventricular fibrillation [VT/VF], hemodynamically unstable sustained VT)
Secondary prevention (cardiac arrest survivors of ventricular tachycardia/ventricular fibrillation [VT/VF], hemodynamically unstable sustained VT)
 Structural heart disease and sustained VT, whether hemodynamically stable or unstable
Structural heart disease and sustained VT, whether hemodynamically stable or unstable

 LVEF less than or equal to 35% at least 40 days after MI and NYHA functional class II-III
LVEF less than or equal to 35% at least 40 days after MI and NYHA functional class II-III
 LVEF less than 30% at least 40 days after MI and NYHA functional class I
LVEF less than 30% at least 40 days after MI and NYHA functional class I


 ICD therapy is recommended to improve survival in patients who have survived cardiac arrest or who have sustained VT, which is either poorly tolerated or associated with reduced systolic LV function (class I; level of evidence A).
ICD therapy is recommended to improve survival in patients who have survived cardiac arrest or who have sustained VT, which is either poorly tolerated or associated with reduced systolic LV function (class I; level of evidence A).


Bibliography, Suggested Readings, and Websites
1. Arnold, J.M.O., Heart Failure (HF) 2012 Available at http://www.merckmanuals.com/professional/cardiovascular_disorders/heart_failure/heart_failure_hf.html Accessed March 19, 2013
2. Cooper, L.T., Baughman, K.L., Feldman, A.M., et al. The role of endomyocardial biopsy in the management of cardiovascular disease: a scientific statement from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology. Endorsed by the Heart Failure Society of America and the Heart Failure Association of the European Society of Cardiology. J Am Coll Cardiol. 2007;50:1914–1931.
3. Epstein, A.E., DiMarco, J.P., Ellenbogen, K.A., et al. ACC/AHA/HRS 2008 guidelines for device-based therapy of cardiac rhythm abnormalities: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices) developed in collaboration with the American Association for Thoracic Surgery and Society of Thoracic Surgeons. J Am Coll Cardiol. 2008;51:e1–e62.
4. Heart Failure Society of America. The HFSA website. Available at http://www.hfsa.org. Accessed March 19, 2013
5. Heart Failure Society of America. Heart failure in patients with left ventricular systolic dysfunction. J Card Fail. 2006;12:e38–e57.
6. Hunt, S.A., Abraham, W.T., Chin, M.H., et al. ACC/AHA 2005 guideline update for the diagnosis and management of chronic heart failure in the adult: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure). J Am Coll Cardiol. 2005;46:e1–e82.
7. Jessup, M., Abraham, W.T., Casey, D.E., et al. Focused Update: ACCF/AHA Guidelines for the Diagnosis and Management of Heart Failure in Adults. Circulation. 2009;119:1977–2016.
8. Mann, D.L. Management of heart failure patients with reduced ejection fraction. In Libby P., Bonow R., Mann D., eds.: Braunwald’s heart disease: a textbook of cardiovascular medicine, ed 8, Philadelphia: Saunders, 2008.
9. Swedberg, K., Cleland, J., Dargie, H., et al. Guidelines for the diagnosis and treatment of chronic heart failure: executive summary (update 2005): the Task Force for the Diagnosis and Treatment of Chronic Heart Failure of the European Society of Cardiology. Eur Heart J. 2005;26:1115–1140.
10. Dumitru, I. Heart Failure. Available at http://www.emedicine.com. Accessed March 19, 2013


