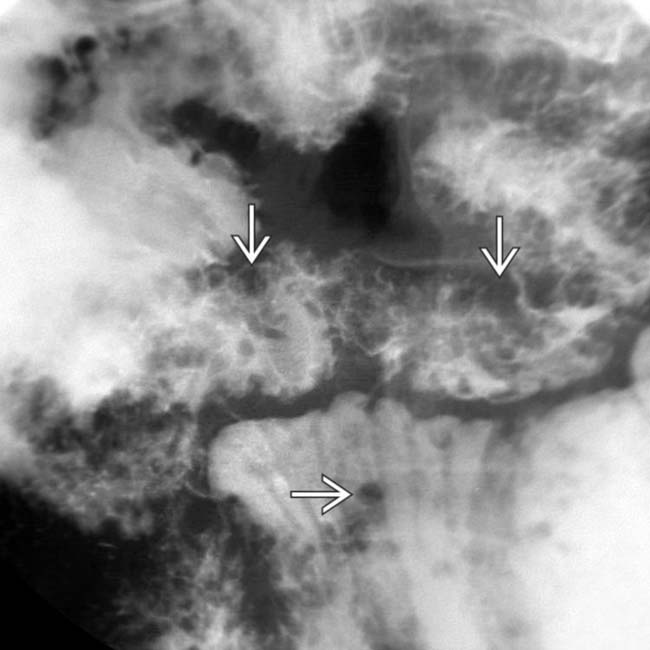
[level-membership-for-radiology-category] Cluster of small filling defects in small bowel with intussusception






 , presumably hamartomas, throughout his bowel.
, presumably hamartomas, throughout his bowel.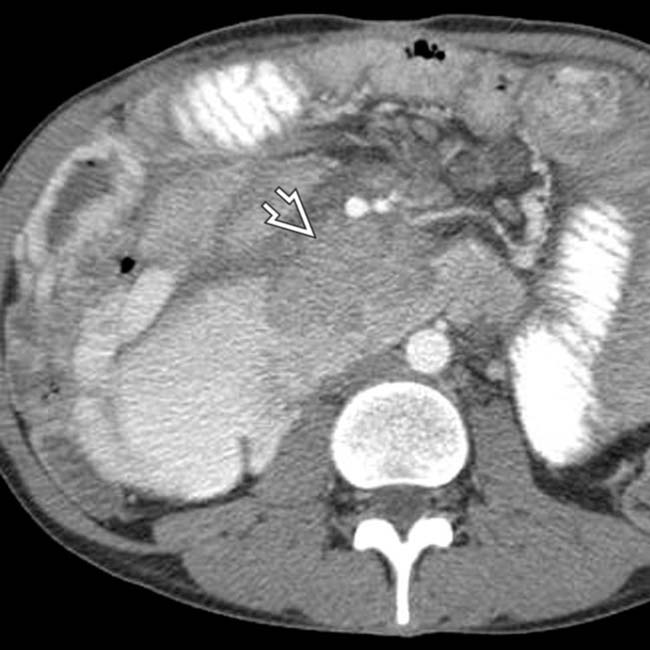
 causing partial obstruction of the duodenum. The mass proved to be a metastasis from a testicular nonseminomatous germ cell tumor.
causing partial obstruction of the duodenum. The mass proved to be a metastasis from a testicular nonseminomatous germ cell tumor.
 , probably due to the hamartomatous polyps.
, probably due to the hamartomatous polyps.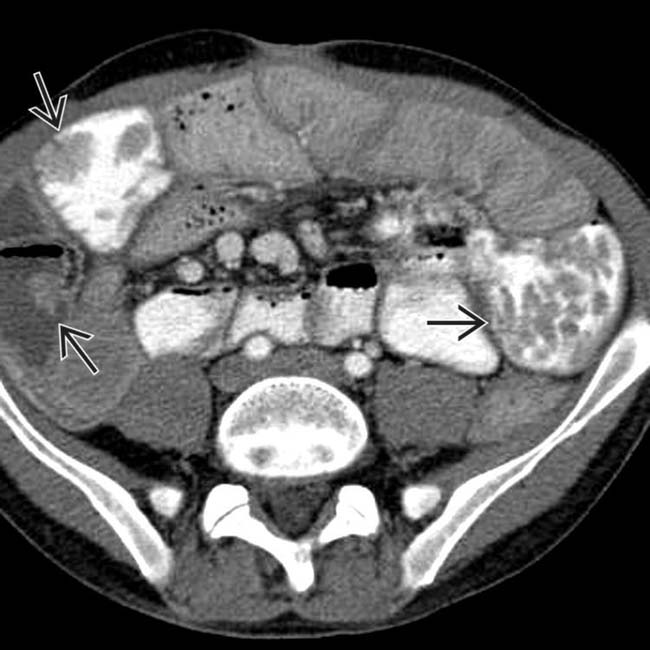
 . As illustrated by this case, some patients with PJS may develop malignant tumors, not just of the bowel, but also of the breast, pancreas, or reproductive tract.
. As illustrated by this case, some patients with PJS may develop malignant tumors, not just of the bowel, but also of the breast, pancreas, or reproductive tract.
































 proven at surgery to be due to hamartomatous polyps.
proven at surgery to be due to hamartomatous polyps.
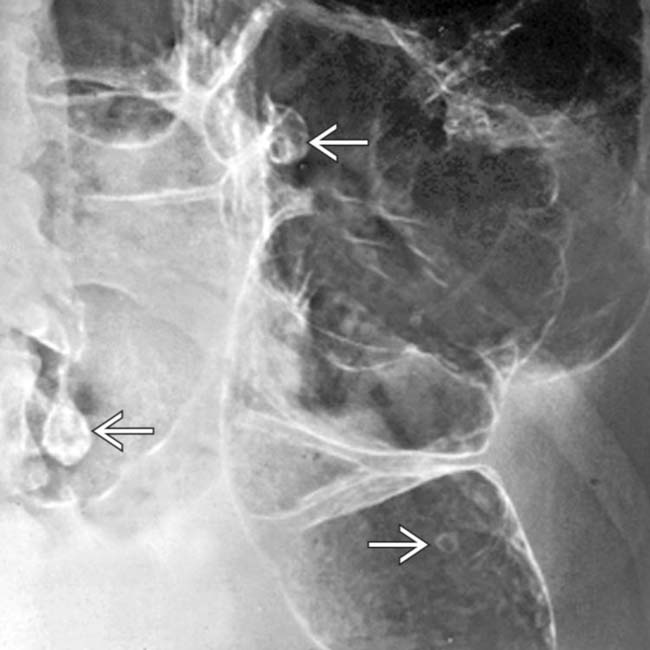
 in a patient with Peutz-Jeghers syndrome.
in a patient with Peutz-Jeghers syndrome.
[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Cluster of small filling defects in small bowel with intussusception
, presumably hamartomas, throughout his bowel. causing partial obstruction of the duodenum. The mass proved to be a metastasis from a testicular nonseminomatous germ cell tumor., probably due to the hamartomatous polyps.. As illustrated by this case, some patients with PJS may develop malignant tumors, not just of the bowel, but also of the breast, pancreas, or reproductive tract.IMAGING
General Features
Radiographic Findings
Buy Membership for Radiology Category to continue reading. Learn more here
[/not-level-membership-for-radiology-category]
