116 Haemochromatosis
Salient features
History

Advanced-level questions
How would you confirm your diagnosis?
• Transferrin saturation is increased
• Serum ferritin levels are raised
• Liver biopsy to measure iron stores is a definitive test
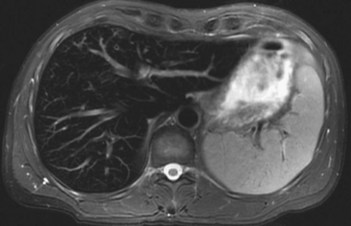
• MRI is now the modality of choice for non-invasive quantification of iron storage in the liver. It allows repeated measurements and reduces sampling errors (Fig. 116.2).
How would you manage such a patient?
• Avoidance of alcohol and Indian balti curries, which are prepared in cast iron cookware (BMJ 1995;310:1368)
• Avoidance of uncooked shellfish and marine fish, since these patients are susceptible to fatal septicaemia from the marine bacterium Vibrio vulnificus
• Phlebotomy: venesection prolongs life and often reverses tissue damage. Initially, weekly venesection (500 ml blood per week) for 2 years (as 50 g iron or more is removed) and then once every 3 months. Iron depletion is confirmed by serum ferritin <50 µg/l and transiferrin saturation <40%. Many manifestations improve (insulin requirements often diminish) except for testicular atrophy and chrondrocalcinosis
• Deferoxamine, an iron chelating agent is used when haemodynamics do no permit venesection
• Screening of family members by measuring fasting transferring saturation and ferritin levels.
Mention a few causes of generalized pigmentation
Common causes are sun tan and race.
The term haemochromatosis was first used by von Recklinghausen (p. 279) in 1889 to describe postmortem findings in men with cirrhosis associated with massive deposition of iron in the hepatocytes (von Recklinghausen FD Ueber Hämochromatose. Tageblatt Versamml Dtsch Naturforsch Artze Heidelberg 1889;62:324–5).
The inherited nature of haemochromatosis was first recognized by Sheldon in 1935.