Chapter 7 Gynaecological Infections
Vaginal discharge and infection
Source of vaginal discharge
Vulva: Greater vestibular glands, glands of vulval skin.
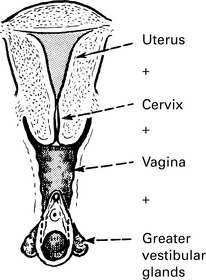
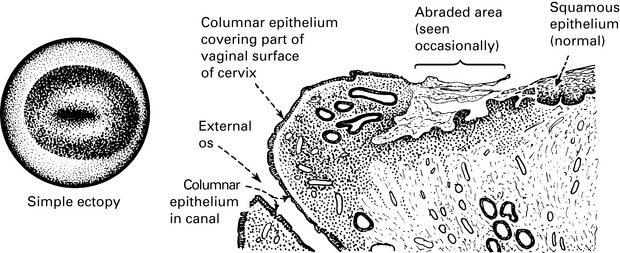
Cervix: Alkaline mucous secretion which becomes copious and watery during ovulation.
Complaints of vaginal discharge
Women will complain under the following conditions.
Examination
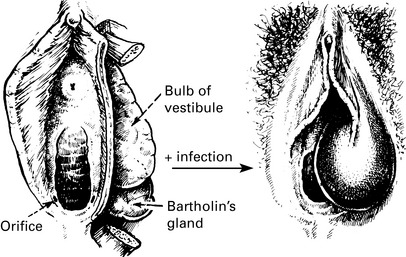
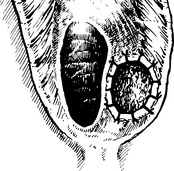
1. Vulva, perineum and thighs are inspected for signs of excoriation. The vestibular glands and urethral meatus are observed and palpated.
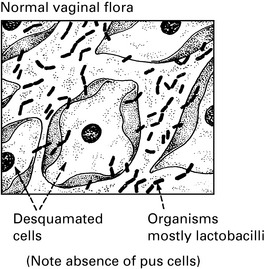
Vaginal discharge
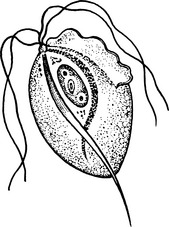
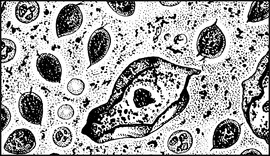
Candida albicans
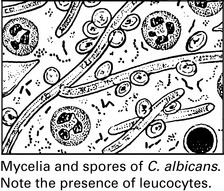
Source of Infection
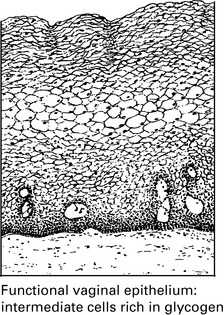
1. Pregnancy. The vagina provides a tropical microclimate and the high concentration of sex steroids in the blood maintains an increased glycogen formation in the vaginal epithelium and may alter the local pH.
2. Immunosuppressive therapy. This includes cytotoxic drugs and corticosteroids. There is also thought to be a natural degree of immunosuppression during pregnancy.
Vaginitis
Vulvovaginitis in children
With reference to the above points.
(a) the changes will be those of physical damage to the tissues. Infection will depend to some extent on whether the person guilty of the offence is a carrier of a specific agent.
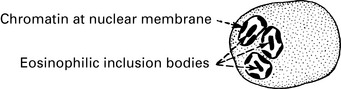
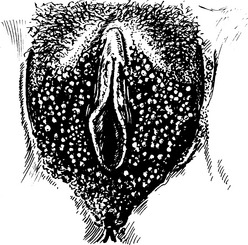
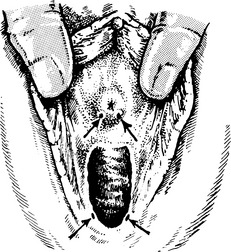
Genital herpes
Clinical findings
Infection of the neonate can lead to herpes encephalitis with a primary infection.

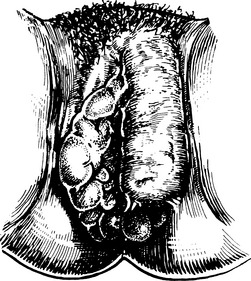
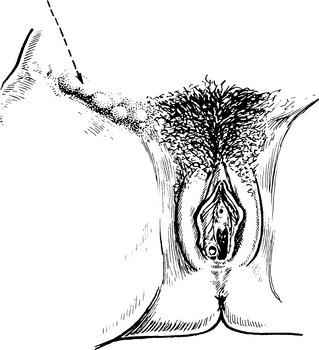
Genital warts
Differential diagnosis
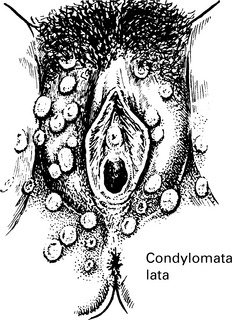
1. Syphilitic condylomata. These are more widespread and not confined to the genital area. They are also flatter and more rounded. Treponemes can be found in the tissue fluid. Serological tests will of course confirm the diagnosis.
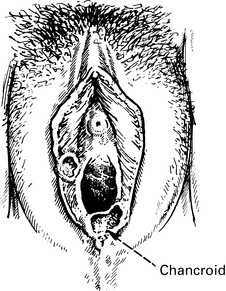
Bacterial infections
Tropical sexually transmitted infections
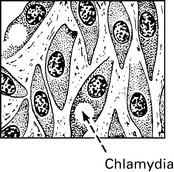
Lymphogranuloma venereum (LGV)
LGV is attributed to a strain of Chlamydia. This is rare in the developed countries.
Gonorrhoea

Syphilis
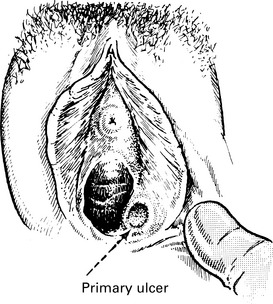
Diagnosis of syphilis
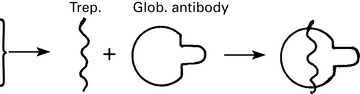

Signs and symptoms of syphilis
Diagnosis is by the demonstration of T. pallidum in the lesions and by serological tests.
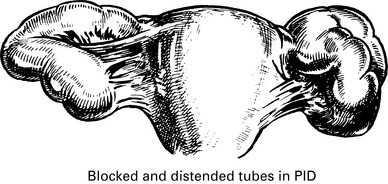
Pelvic inflammatory disease
Differential diagnosis
Pelvic inflammatory disease

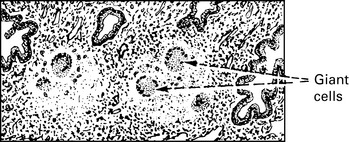
Genital tuberculosis
Diagnosis
Human immunodeficiency virus
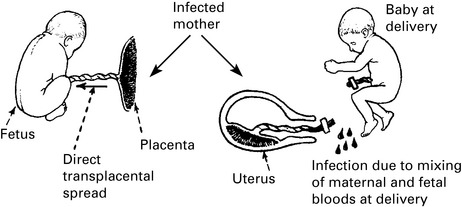
Transmission
The following are the main modes of transmission of human immunodeficiency virus (HIV):
• Injection or transfusion of contaminated blood or blood products, donations of semen (artificial insemination), skin grafts or organ transplants taken from someone who is infected.
• From a mother who is infected to her baby; this can occur during pregnancy, at birth and through breastfeeding.
Acquired immune deficiency syndrome (AIDS)
Three conditions are particularly characteristic of the immunodeficiency state:
Intercurrent infections frequently found in aids patients
| Infective agents | Clinical results |
|---|---|
| Parasites | |
| Pneumocystis carinii | Pneumonia |
| Cryptosporidium | Severe diarrhoea |
| Strongyloides stercoralis | Severe diarrhoea |
| Toxoplasma gondii | Chorio-retinitis |
| Viruses | |
| Herpes | Pneumonia |
| J.C. virus | Leuco-encephalopathy |
| Bacteria | |
| Species usually causing minor lesions, e.g. skin spots | Septicaemia |
| Fungi | |
| Cryptococcus neoformans | Pneumonia, meningitis |