Chapter 43 GRANULOMATOUS LIVER DISEASE
PRESENTATION AND CLINICAL EXAMINATION
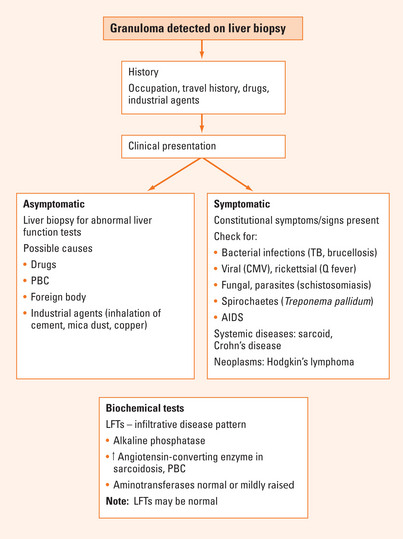
Typical presentations include pyrexia of unknown origin or incidental abnormal liver function tests. Often the clinical examination is normal, though there may be symptoms and signs of an associated systemic disease (Figure 43.1). Infrequently, hepatomegaly, splenomegaly or lymphadenopathy may be detected.
Biochemical liver tests
Generally, liver function testing is non-specific, but a predominant alkaline phosphatase (ALP) elevation may be present.
Histopathology
Hepatic granulomas are found in 0.8%–15% of liver biopsies. The epithelioid granuloma may be associated with distinguishing morphological pathological features. These can include duct involvement (primary biliary cirrhosis), periductal location with acute inflammatory changes (large duct obstruction with cholangitis), parenchymal and perivenular location (tuberculosis), caseation (tuberculosis), fibrin-ring pattern with central fat vacuole (Q fever), schistosome ova (schistosomiasis) or a positive fungal stain.
CAUSES OF GRANULOMAS
The most common causes of hepatic granulomas where primary biliary cirrhosis has been excluded are sarcoidosis, chronic liver disease, biliary tract disease, tuberculosis, Q fever, other infections, drug hepatotoxicity, neoplasms and idiopathic (Table 43.1).
| Associated with pyrexia of unknown origin | Sarcoidosis, tuberculosis (miliary and pulmonary, caseation important), atypical mycobacterium, Q fever, brucellosis, cat-scratch disease, mycoses, drugs, idiopathic granulomatous hepatitis |
| Human immunodeficiency virus (HIV) | Mycobacterium avium complex, idiopathic, other mycobacteria, Mycobacterium tuberculosis, Cryptococcus, Histoplasma, medications (trimethoprim-sulfamethoxazole) |
| Infectious diseases | Bacteria: actinomycosis, brucellosis, cat-scratch disease, listeriosis, syphilis, tularaemia, Whipple’s disease |
| Mycobacteria: tuberculosis, leprosy (lepromatous and tuberculoid) | |
| Rickettsia: Q fever | |
| Chlamydia: lymphopathia venereum, psittacosis | |
| Fungi: aspergillosis, blastomycosis, candidiasis, cryptococcosis, histoplasmosis | |
| Viruses: cytomegalovirus, Epstein-Barr virus, infectious mononucleosis | |
| Parasites: amoebiasis, capillariasis, fascioliasis, schistosomiasis, toxoplasmosis, visceral leishmaniasis (kala-azar) | |
| Hypersensitivity and immunological diseases | Metals: beryllium, copper, gold |
| Hypogammaglobulinaemia, primary biliary cirrhosis, primary sclerosing cholangitis, systemic lupus erythematosus | |
| Vascular diseases: disseminated visceral giant cell arteritis, polyarteritis nodosa, temporal arthritis, Wegener’s granulomatosis | |
| Foreign materials | Anthracotic pigments, barium, cement and mica dust; mineral oil—radiocontrast media, food additives; silica, suture material, talc |
| Neoplasms | Hodgkin’s disease, non-Hodgkin’s lymphoma |
| Miscellaneous diseases | Biliary tract obstruction, bile granulomas, chronic inflammatory bowel disease, eosinophilic gastroenteritis, jejunoileal bypass, porphyria cutanea tarda, sarcoidosis, idiopathic |
| Drugs | Allopurinol, amiodarone, amoxicillin/clavulanic acid, chlorpromazine, chlorpropamide, diltiazem, gold salts, halothane, hydralazine, methyldopa, benzylpenicillin, phenoxymethylpenicillin, phenylbutazone, phenytoin, procainamide, quinidine, quinine, sulfonamides |
Primary biliary cirrhosis
Epidemiological, clinical and biochemical features
Kaplan MM, Gershwin ME. Primary biliary cirrhosis. N Engl J Med. 2005;353:1261-1273.
Knox TA, Kaplan MM, Golfand JA, et al. Methotrexate treatment of idiopathic granulomatous hepatitis. Ann Int Med. 1995;122:592-595.
Lefkowitch JH. Hepatic granulomas. J Hepatol. 1999;30:40-45.
Matheus T, Muñoz S. Granulomatous liver disease and cholestasis. Clin Liver Dis. 2004;8:229-246.
Sandor M, Weinstock JV, Wynn TA. Granulomas in schistosome and mycobacterial infections: a model of local immune responses. Trends Immunol. 2003;24:44-52.






